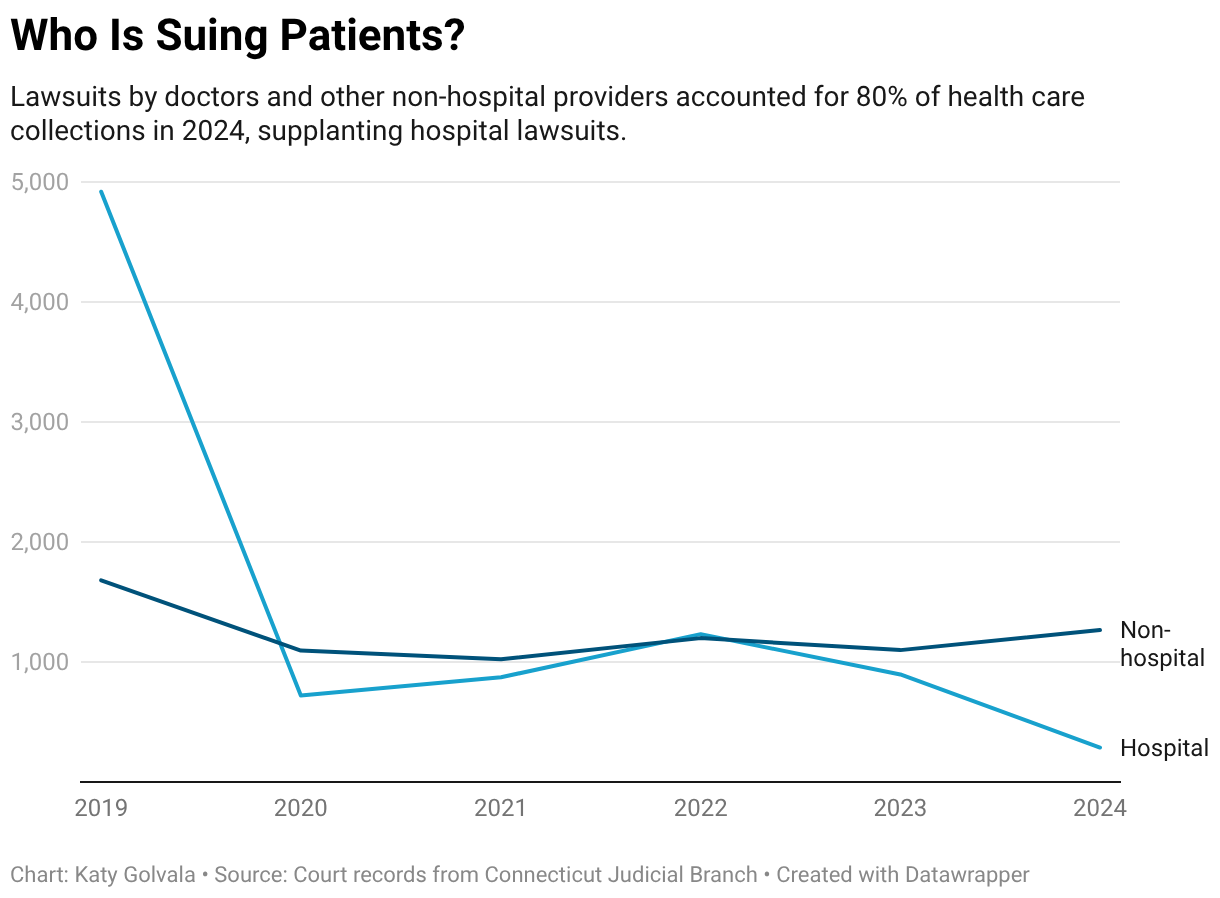
In Connecticut, Doctors Now Sue Patients Most Over Medical Bills, Surpassing Hospitals
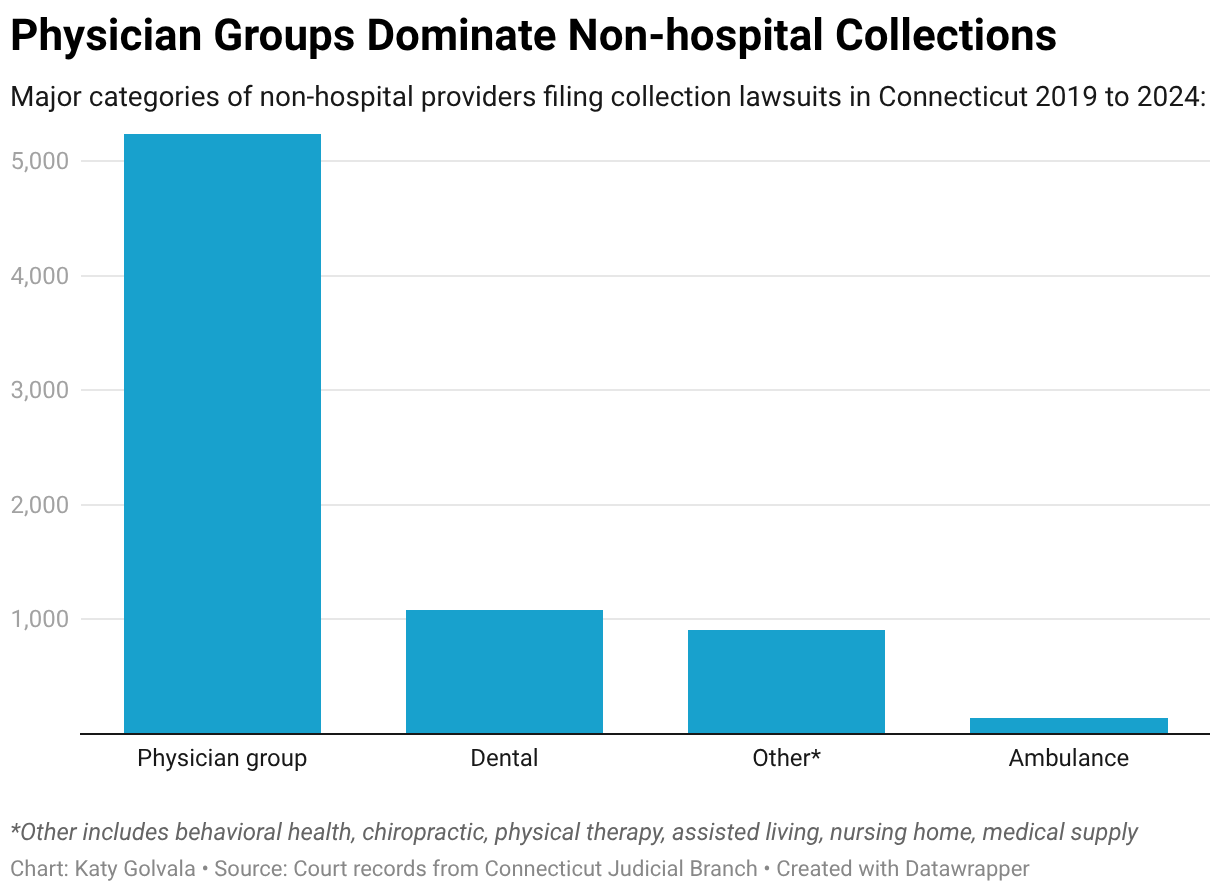
Physicians, dentists, and other nonhospital providers account for more than 80% of health care debt collection cases in Connecticut courts, a CT Mirror-┬ķČ╣┼«ė┼ Health News investigation finds.