Baltimore's Other Divide Archives - Â鶹ŮÓÅ Health News
/series/baltimore-other-divide/
Â鶹ŮÓÅ Health News produces in-depth journalism on health issues and is a core operating program of Â鶹ŮÓÅ.Thu, 16 Apr 2026 04:09:16 +0000en-US
hourly
1 https://wordpress.org/?v=6.8.5/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=32Baltimore's Other Divide Archives - Â鶹ŮÓÅ Health News
/series/baltimore-other-divide/
3232161476233Hospitals Find Asthma Hot Spots More Profitable To Neglect Than Fix
/public-health/hospitals-find-asthma-hot-spots-more-profitable-to-neglect-than-fix/
Wed, 06 Dec 2017 10:02:35 +0000BALTIMORE — Keyonta Parnell has had asthma most of his young life, but it wasn’t until his family moved to the 140-year-old house here on Lemmon Street two years ago that he became one of the health care system’s frequent customers.
“I call 911 so much since I’ve been living here, they know my name,” said the 9-year-old’s mother, Darlene Summerville, who calls the emergency medical system her “best friend.”
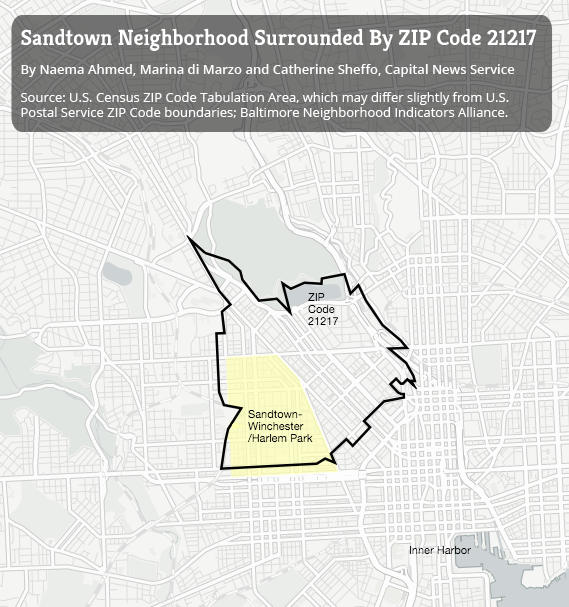
Summerville and her family live in the worst asthma hot spot in Baltimore: ZIP code 21223, where decrepit houses, rodents and bugs trigger the disease and where few community doctors work to prevent asthma emergencies. One mom there wields a BB gun to keep rats from her asthmatic child.
Residents of this area visit hospitals for asthma flare-ups at more than four times the rate of people from the city’s wealthier neighborhoods, according to data analyzed by Kaiser Health News and the University of Maryland’s Capital News Service.
Baltimore paramedic crews make more asthma-related visits per capita in 21223 than anywhere else in the city, according to fire department records. It is the second-most-common ZIP code among patients hospitalized for asthma, which, when addressed properly, should never require emergency visits or hospitalization.
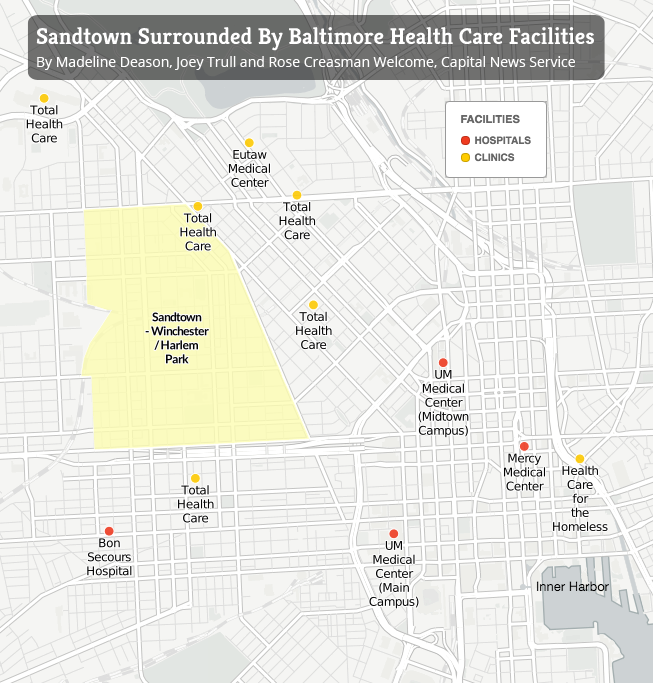
The supreme irony of the localized epidemic is that Keyonta’s neighborhood in southwest Baltimore is in the shadow of prestigious medical centers — Johns Hopkins, whose researchers are international experts on asthma prevention, and the University of Maryland Medical Center.
Both receive massive tax breaks in return for providing “community benefit,” a poorly defined federal requirement that they serve their neighborhoods. Under Maryland’s ambitious effort to control medical costs, both are supposed to try to improve residents’ health outside the hospital and prevent admissions.
But like hospitals across the country, the institutions have done little to address the root causes of asthma. The perverse incentives of the health care payment system have long made it far more lucrative to treat severe, dangerous asthma attacks than to prevent them.
Hopkins, UMMC and other hospitals collected $84 million over the three years ending in 2015 to treat acutely ill Baltimore asthma patients as inpatients or in emergency rooms, according to the news organizations’ analysis of statewide hospital data. Hopkins and a sister hospital received $31 million of that.
Executives at Hopkins and UMMC acknowledge that they should do more about asthma in the community but note that there are many competing problems: diabetes, drug overdoses, infant mortality and mental illness among the homeless.
Science has shown it’s relatively easy and inexpensive to reduce asthma attacks: Remove rodents, carpets, bugs, cigarette smoke and other triggers. Deploy community doctors to prescribe preventive medicine and health workers to teach patients to use it.
Ben Carson, secretary of the Department of Housing and Urban Development, who saw hundreds of asthmatic children from low-income Baltimore during his decades as a Hopkins neurosurgeon, said that the research on asthma triggers is unequivocal. “It’s the environment — the moist environments that encourage the mold, the ticks, the fleas, the mice, the roaches,” he said in an interview.
Research showing that removing household triggers reduces asthma attacks “is unequivocal,” says Ben Carson, a former Johns Hopkins neurosurgeon and now secretary of the Department of Housing and Urban Development. “The cost of not taking care of people is probably greater than the cost of taking care of them.” (Katherine Gilyard/KHN)
As the leader of HUD, he says he favors reducing asthma risks in public housing as a way of cutting expensive hospital visits. The agency is discussing ways to finance pest removal, moisture control and other remediation in places asthma patients live, a spokeswoman said.
“The cost of not taking care of people is probably greater than the cost of taking care of them” by removing triggers, Carson said, adding, “It depends on whether you take the short-term view or the long-term view.”
The Long View
Asthma is the most common childhood medical condition, with rates who often live in run-down homes, than among kids in wealthier households. The disease causes nearly in the United States a year, about and thousands of deaths annually.
That drives the total annual cost of asthma care, including medicine and office visits, .
Keyonta lives in a two-bedroom row house on the 1900 block of Lemmon Street, which some residents call the “Forgetabout Neighborhood,” about a mile from UMMC and 3 miles from Hopkins.
Reporters spent months interviewing patients and parents and visiting homes in 21223, a multiracial community where the average household income of $38,911Â is lower than in all but two other ZIP codes in Maryland.
To uncover the impact of asthma, the news organizations analyzed every Maryland inpatient and emergency room case over more than three years through a special agreement with the state commission that sets hospital rates and collects such data. The records did not include identifying personal information.
For each emergency room visit to treat Baltimore residents for asthma, according to the data, hospitals were paid $871, on average. For each inpatient case, the average revenue was $8,698. In one recent three-year period, hospitals collected $6.1 million for treating just 50 inpatients, the ones most frequently ill with asthma, each of whom visited the hospital at least 10 times.
Lemmon Street’s trash piles and vacant homes harbor rodents and insects that can set off asthma flare-ups. (Doug Kapustin for KHN)
Darlene Summerville partly blames a moldy dirt basement for triggering her children’s asthma flare-ups. (Doug Kapustin for KHN)
shows that shifting dollars from hospitals to Lemmon Street and other asthma hot spots could more than pay for itself. Half the cost of one admission — a few thousand dollars — could buy air purifiers, pest control, visits by community health workers and other measures proven to slash asthma attacks and hospital visits by frequent users.
“We love” these ideas, and “we think it’s the right thing to do,” said Patricia Brown, a senior vice president at Hopkins in charge of managed care and population health. “We know who these people are. . . . This is doable, and somebody should do it.”
But converting ideas to action hasn’t happened at Hopkins or much of anywhere else.
One of the few hospitals making a substantial effort, Children’s National Health System in Washington, D.C., has found that its good work comes at a price to its bottom line.
Children’s sends asthma patients treated in the emergency room to that teaches them and their families how to take medication properly and remove home triggers. The program, begun in the early 2000s, cut emergency room use and other unscheduled visits by those patients by 40 percent, a study showed.
While recognizing that it decreases potential revenue, hospital managers fully support the program, said Dr. Stephen Teach, the pediatrics chief who runs it.
“‘Asthma visits and admissions are down again, and it’s all your fault!’” Children’s chief executive likes to tease him, Teach said. “And half his brain is actually serious, but the other half of his brain is celebrating the fact that the health of the children of the District of Columbia is better.”
I call 911 so much since I’ve been living here, they know my name.
Darlene Summerville
The Close-Up View
Half of the 32 row houses on Summerville’s block of Lemmon Street are boarded up, occupied only by the occasional heroin user. At least 10 people on the block had asthma late last year, according to interviews with residents then.
“We have mold in our house” and a leaky roof, said Tracy Oates, 42, who lived across the street from Summerville. “That is really big trouble as far as triggering asthma.”
Two of her children have the disease. “I don’t even want to stay here,” she said. “I’m looking for a place.”
Shadawnna Fews, 30, lived with her asthmatic toddler on Stricker Street, a few blocks east. She kept a BB gun to pick off rats that doctors said can set off her son’s wheezing.
Delores Jackson, 56, who lived on Wilkens Avenue, a few blocks south of Lemmon Street, said she had been to the hospital for asthma three times in the previous month.
All three of Summerville’s kids have asthma. Before moving to Lemmon Street two years ago, she remembers, Keyonta’s asthma attacks rarely required medical attention.
But their new house contained a clinical catalog of asthma triggers.
The moldy basement has a dirt floor. Piles of garbage in nearby vacant lots draw vermin: mice, which are , along with rats. Summerville, 37, kept a census of invading insects: gnats, flies, spiders, ants, grasshoppers, “little teeny black bugs,” she laughed.
Often she smokes inside the house.
The state hospital data show that about 25 Marylanders die annually from acute asthma, their airways so constricted and blocked by mucus that they suffocate.
Keyonta missed dozens of school days last year because of his illness, staying home so often that Summerville had to quit her cooking job to care for him. Without that income, the family nearly got evicted last fall and again in January. The rent is $750.
About a third of Baltimore high school students report they have had asthma, causing frequent absences and missed learning, said Dr. Leana Wen, Baltimore’s health commissioner.
With numbers like that, West Baltimore’s primary care clinics, which treat a wide range of illnesses, as is the city health department’s asthma program, whose three employees visit homes of asthmatic children to demonstrate how to take medication and reduce triggers.
The program, which an analysis by Wen’s office showed cut asthma symptoms by 89 percent, “is chronically underfunded,” she said. “We’re serving 200 children [a year], and there are thousands that we could expand the program to.”
‘The Hospital Instead Of The Classroom’
The federal government paid for $1.3 billion in asthma-related research over the past decade, of which $205 million went to Hopkins, records show. The money supports basic science as well as many studies showing that modest investments in community care and home remediation can improve lives and save money.
“Getting health care providers to pay for home-based interventions is going to be necessary if we want to make a dent in the asthma problem,” said Patrick Breysse, a former Hopkins official, who as director of the National Center for Environmental Health at the Centers for Disease Control and Prevention is one of the country’s top public health officials.
Other factors can trigger asthma: outdoor air pollution and pollen, in particular. But eliminating home-based triggers could , one study showed.
Perhaps no better place exists to try community asthma prevention than Maryland. By guaranteeing hospitals’ revenue each year, the state’s unique rate-setting system encourages them to cut admissions with preventive care, policy authorities say.
But Hopkins, UMMC and their corporate parents, whose four main Baltimore hospitals together collect some $5 billion in revenue a year, have so far limited their community asthma prevention to small, often temporary efforts, often financed by somebody else’s money.
UMMC’s Breathmobile program, which visits Baltimore schools dispensing asthma treatment and education, depends on outside grants and could easily be expanded with the proper resources, said its medical director, Dr. Mary Bollinger. “The need is there, absolutely,” she said.
Hopkins runs “Camp Superkids,” a weeklong, sleep-away summer session for children with asthma that costs participants $400, although it awards scholarships to low-income families. It’s also conducting yet another study — testing referral to follow-up care for emergency room asthma patients, which Children’s National long ago showed was effective.
But no hospital has invested substantially in home remediation to eliminate triggers, a proven strategy supported by the HUD secretary and promoted by Green and Healthy Homes Initiative, a Baltimore nonprofit that works to reduce asthma and lead poisoning.
“We either go forward to do what has been empirically shown to work, or we continue to bury our heads in the sand and kids will continue to go to the hospital instead of the classroom,” said Ruth Ann Norton, the nonprofit’s chief executive.
Hopkins and UMMC say they do plenty to earn their community benefit tax breaks.
“It’s always a challenge to say, ‘Where do we start first?’” said Dana Farrakhan, a senior vice president at UMMC whose duties include community health improvement.
Among other initiatives, UMMC takes credit for working with city officials to sharply reduce infant mortality by working with expectant mothers. The organization’s planned outpatient center will include health workers to help people reduce home asthma triggers, Farrakhan said.
“What we do is perhaps not sufficiently focused,” Brown of Hopkins said. At the same time, “we have to have revenue,” she said. “We’re a business.”
After months of waiting, Summerville considered herself lucky to get an appointment with the city health department’s asthma program.
One of its health workers came to the house late last year. She supplied mousetraps and mattress and pillow covers to control mites and other triggers. She helped force Summerville’s landlord to fix holes in the ceiling and floor.
She urged Summerville to stop smoking inside and gave medication lessons, which uncovered that Summerville had mixed up a preventive inhaler with the medicine used for Keyonta’s flaring symptoms.
“The asthma lady taught me what I needed to know to keep them healthy,” Summerville said of her family.
That was late in 2016. Since then, Summerville said last month, she hasn’t called an ambulance.
METHODOLOGY:
Kaiser Health News and the University of Maryland’s Capital News Service obtained data held by the Maryland Health Services Cost Review Commission on every hospital inpatient and emergency room case in the state from mid-2012 to mid-2016 — some 10 million cases. The anonymized data did not include identifying personal information.
The news organizations measured asthma costs by calculating total charges for cases in which asthma was the principal diagnosis. Maryland’s hospital rate-setting system ensures that such listed charges are very close to equaling the payments collected.
To determine asthma prevalence, reporters calculated the per capita rate of hospital visits with asthma as a principal diagnosis — a method frequently used by health departments and researchers. This may exaggerate asthma prevalence in low-income ZIP codes such as 21223, because of those communities’ tendency to use hospital services at greater rates.
However, the data also point to high asthma rates in 21223 and other low-income Baltimore communities — for example, asthma prevalence within the population of all hospital patients in a ZIP code.
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=793426&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>793426Attack On Asthma: Scrubbing Homes Of Allergens May Tame Disease And Its Costs
/public-health/attack-on-asthma-scrubbing-homes-of-allergens-can-tame-disease-and-its-costs/
Wed, 06 Dec 2017 10:00:49 +0000After years of studying the causes of asthma, a pediatrician-turned-public health sleuth thinks there’s a way to substantially reduce its impact.
But the approach faces a big hurdle: getting someone to pay for it, said Dr. Elizabeth Matsui, a professor at Johns Hopkins medical school in Baltimore.
Matsui, who suffered from asthma as a child, has spent much of her career studying the link between poor housing and asthma in low-income neighborhoods. In particular, she’s looked at the effects of mouse allergens, typically found in high concentrations in urban homes.
Matsui cited a 2004 study in the New England Journal of Medicine that described measures to reduce home allergen levels and concluded that they were linked to reductions in asthma symptoms.
That research “was highly successful and impactful,” but the approach wasn’t widely adopted, Matsui said.
“So here we have this trial that was published more than 10 years ago that shows [indoor allergen control] works,” said Matsui, who did not participate in the study. “But the families who need it most can’t afford to do these things, don’t have control oftentimes over their home environment, and insurance or other payers don’t cover these things.”
Matsui has proposed new incentives for hospitals to provide home intervention, including Medicaid waivers. But, she said, scientists can’t use research money for these programs. “Delivery of community health care programs would require a different type of funding.”
As a result, doctors and scientists doubted if a plan to control home allergens would scale up, and insurers questioned whether benefits to their bottom line would justify the added cost.
“We have this enormous public health problem in that there are housing conditions that directly affect allergen exposure in this population of kids,” Matsui said. “We have dedicated individuals and groups who are trying to solve the problem. But we don’t have a system that is able to solve the problem.”
A by Matsui, published in the Journal of the American Medical Association, suggests that even without intensive professional cleaning services, families that receive some training can substantially reduce home allergens on their own.
That finding suggests health agencies should routinely offer to educate asthma-affected families in home allergen control. “There’s potentially a large benefit,” Matsui said.
In a separate study, Matsui’s group is following 200 Baltimore children to see if those in homes scrubbed of allergens need fewer treatments with rescue inhalers. If they do, that could give health insurers an incentive to pay for the approach.
There’s another incentive: Clearing the air in a child’s home may be critical in cases where medications alone don’t work. “We continue to see a lot of kids that, despite being on medication, don’t have well-controlled asthma,” Matsui said.
Asthma drugs can also have serious side effects, she said, especially at higher doses, and may suppress symptoms without halting lung damage.
Matsui’s work on asthma began while working as a pediatrician at Baltimore’s Franklin Square Hospital in 1998. As part of her job, she spent half a day each week in a school health clinic in a low-income area.
Matsui was struck by the number of kids she saw with severe asthma, she said, and set up a home health visit program to help them. But she wasn’t certain the program was working, so she consulted with experts at Hopkins.
In 2004, she earned a master’s from the Hopkins school of public health. Today, she is one of the nation’s leading asthma researchers.
Matsui said her career was shaped by her own struggle with childhood asthma. “I think that that probably played a role, consciously or unconsciously,” she said.
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=741260&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>741260Baltimore Draws 10-Year Blueprint To Cut Racial Health Disparities
/public-health/baltimore-draws-10-year-blueprint-to-cut-racial-health-disparities/
Wed, 31 Aug 2016 11:21:04 +0000http://khn.org/?p=654494Baltimore officials presented a 10-year plan Tuesday that sharply highlights the poor health status of African-Americans and aims to bring black rates of lead poisoning, heart disease, obesity, smoking and overdoses more in line with those of whites.
“We wanted to specifically call out disparities” in racial health, said Dr. Leana Wen, who became the city’s health commissioner early last year. “And we have a moonshot. Our moonshot is we want to cut health disparities by half in the next 10 years.”
Black Baltimore leaders praised Wen for putting disparities squarely in the conversation even as they acknowledged the difficulty of achieving the plan’s goals.
“It’s a big challenge. There’s no debating that,” said Diane Bell-McKoy, CEO of Associated Black Charities, a Maryland nonprofit. “She takes a step forward more so than anybody else I’ve seen because she calls it out. Most of the time we find code words for it. We don’t call it out.”
Violence last year following the death of Freddie Gray, a black man who died after being injured in police custody,  as well as its criminal justice differences, officials said. Gray’s family had won a settlement for alleged lead-paint poisoning, which is blamed for low test scores and cognitive challenges among thousands of Baltimore children.
“What happened last year with Freddie Gray put Baltimore in the national media spotlight,” said Helen Holton, a Baltimore councilwoman who represents a portion of the city’s west side. “That made people stop and take notice of what had been going on and stop treating it as business as usual.”
°Õ³ó±ðÌý, called Healthy Baltimore 2020, was  by the Baltimore Sun. Officials plan to track blood-lead levels, overdose deaths, child fatalities, healthy-food availability and other indicators year by year. It’s called Healthy Baltimore 2020 because officials have set ambitious goals to achieve before 10 years is up, Wen said.
Tentative targets include cutting youth homicides by 10 percent and disparities in obesity, smoking and heart-disease deaths by 15 percent — all by 2020.
Tactics include more programs to reduce street violence, expanded anti-smoking campaigns, more home visits for pregnant women and increased access to naloxone, which blocks the effects of heroin.
The blueprint is “an ongoing document” that will be amended with community participation and results closely scored, Wen said.
“Our community is sick of us overpromising and underdelivering,” she said.
Baltimore officials have made substantial progress in ,Ìý±ô´Ç·É±ð°ù¾±²Ô²µÌý and cutting .
But as in many other areas, Baltimore is still divided by health. Residents of Gray’s west-side neighborhood of  live 10 years less on average than Marylanders in general. Poor neighborhoods have far higher rates of heart disease, diabetes, addiction, HIV infection and other illness than more prosperous parts of the city.
Black leaders emphasized that Baltimore’s health won’t improve unless policymakers address deeper causes of illness such as poverty, unemployment and poor housing.
“It is affirming to see someone in Dr. Wen’s role address the uncomfortable truths behind health inequities,” said Debbie Rock, CEO of LIGHT Health and Wellness, which offers health and other community services on Baltimore’s west side. “This is a great platform to also address upstream factors” such as low incomes, she said.
Holton compared the health blueprint to a  alleging a pattern of excessive force and violation of constitutional rights by the Baltimore Police Department.
Both documents address racial differences and offer challenges for improvement, she said.
“You can travel 5Â miles from one neighborhood to another and it’s like you are in two different communities” in health levels, Holton said. “Freddie Gray was like the tipping point. Let’s take this and make it a teachable moment of how to be better moving forward.”
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=654494&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>654494A Young Latina In Baltimore Struggles To Keep Her Family Healthy
/public-health/a-young-latina-in-baltimore-struggles-to-keep-her-family-healthy/
Fri, 08 Jul 2016 09:00:58 +0000http://khn.org/?p=637173Mom Marlene (left) and daughter Nathaly (right) are finally insured with a special program. Younger daughter Stephanie (center) has had more access to care because she is a U.S. citizen. (Mary Wiltenburg for KHN)
Nathaly Uribe works in a busy insurance office in East Baltimore. But while she sells car and home insurance all day, she can’t afford health coverage for herself.
Uribe is a DREAMer, meaning she qualifies for the Obama administration’s “deferred action” program for people who came to this country as small children. Her mother is undocumented and her sister is a citizen.
Reporting for WYPR and Kaiser Health News, Mary Wiltenburg explores how this mix of immigration status and low income have been barriers to health care for the family.
Listen to the radio story below and click  to read more.
The Annie E. Casey Foundation supports KHN’s coverage of health disparities in East Baltimore.
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=637173&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>637173For Many In Baltimore’s Growing Latino Community, Health Care Is A Challenge
/insurance/for-many-in-baltimores-growing-latino-community-health-care-is-a-challenge/
Mon, 27 Jun 2016 09:00:49 +0000http://khn.org/?p=632831Cecilia Ramirez is worried about her weight and troubling symptoms that hint of diabetes, but she won’t seek medical help because she can’t afford it.
“I don’t go to the doctor when I’m sick — it’s too expensive,” she said.
Though she is a sales worker at an insurance agency in Highlandtown, an East Baltimore neighborhood that has seen an influx of Hispanic immigrants in recent years, Ramirez, 23, has no health insurance.
Her predicament is shared by thousands of Hispanic immigrants in East Baltimore, and millions nationally, who cannot afford regular medical services and are uninsured because they lack the benefits attached to legal U.S. residency and citizenship.
Ramirez’s parents came illegally to the U.S. from Mexico when she was 10. Her immigration status now — “lawfully present” — allows her to work and study here without fear of deportation, but she has no path to citizenship. She is ineligible for health coverage under the Affordable Care Act or any public insurance program.
(The Supreme Court’s decision last week in a related immigration case did not change this.)
Her $23,000 annual income would easily qualify her for Medicaid, but only her two young children can get it. Ramirez’s employer can’t afford to offer her private health insurance either, and even if it did, she doubts she could afford it. So, how can Ramirez deal with the hacking from her lungs?
“Vicks VapoRub,” offers her boss, David Rosario, drawing cynical laughter from Ramirez and others in the office.
Latinos, uninsured or not, face many challenges when it comes to finding medical care. Many have trouble speaking and understanding English, are poor and undereducated, or lack transportation. Others come from cultures where health care is a luxury they don’t regularly seek out.
Cecilia Ramirez and her two daughters, Jenny Rodriguez-Ramirez, 7, and Kimberly Gonzalez-Ramirez, 3. The girls qualify for Medicaid because they were born in the U.S., but their mother does not because of her immigration status. (Doug Kapustin for KHN)
But the inability of non-citizens to join affordable health plans remains the primary stumbling block separating people from Mexico, Central America and South America from care.
“What we’re seeing across the country is that the undocumented are one of the most vulnerable groups out there when it comes to insurability,” said Steven Lopez, manager of the health policy project at the National Council of La Raza, the largest Latino advocacy group in the U.S. “The opportunity to get regular health care is the key to finding greater opportunity. If you don’t have your health, you’re not going to progress in life.”
Nationwide, more than 5 million people living in the U.S. illegally are without medical coverage, with indications that most are Hispanic, according to an released in March. Nearly half of all immigrants living here without permission are uninsured, compared with 10.5 percent of U.S. citizens and roughly 15 percent of non-citizens living here legally, the report noted. Hispanic adults’ uninsured rate fell to 28 percent last year — 13 percentage points below 2013 — but remains far higher than those of non-Hispanic whites, blacks and Asians, according to released in May.
“This is the tricky part for us,” said Leana Wen, Baltimore’s health commissioner. “The Affordable Care Act excludes these individuals” who lack authorization to live in the U.S. “They fall through the cracks.”
They have done so even as Mayor Stephanie Rawlings-Blake works to draw more immigrants here in the hope they will repopulate hollowed out inner-city blocks. Latinos, who figure prominently in the mayor’s drive to recruit 10,000 new families, continue to filter into several older East Baltimore neighborhoods, including Fells Point, Greektown, Highlandtown and Patterson Park.
Baltimore’s population includes around 30,000 Latinos, up from just 9,000 15 years ago, city officials say. Medical providers and Latino advocates say that 40 to 60 percent of them live in the U.S. illegally, a range close to the Urban Institute’s national estimates.
Health is a major concern. Baltimore Latinos are twice as likely as non-Latinos to say they have poor or fair health, according to a in 2011.
There is insufficient data to make judgments about the health of the city’s Latinos or compare them to other groups. But death from cardiovascular disease and cancer were the two leading causes of death among the city’s Latinos in 2012, according to a 2014 report by the department. Unintentional injury and chronic liver disease or cirrhosis tied for the fourth leading cause of death among the city’s Latinos, but they were much less common among white and black populations, the report found.
“People can start businesses and buy homes, but they can’t get medical insurance,” said Rosario, who serves as board president for the Latino Providers Network, an organization that links Hispanics to services.
Working out of an office within Johns Hopkins Hospital’s Bayview Medical Center in Baltimore, Centro SOL social worker Flor Giusti converses with Latino patients in her office there. (Doug Kapustin for KHN)
As a result, health providers say that when they see people come into their offices or clinics, they are often in advanced stages of illness.
“Typically, we see a lot of diabetes and obesity-related diseases, like high blood pressure,” said Kathleen Page, an infectious disease specialist at Johns Hopkins Hospital and a cofounder of Centro SOL, a Bayview outreach program that treats Hispanic clients at reduced prices. Baltimore Latinos suffer higher rates of those disorders despite being younger as a group than the rest of the city’s population. Chronic infections and mental health problems such as anxiety and depression run rampant, Page added.
About 95 percent of the Hispanic patients she sees at her HIV clinic are living here illegally and lack health insurance.
Latinos’ ability to find treatment is tied directly to their immigration status.
Some people in the U.S. without documentation can receive payments for baby deliveries through Emergency Medicaid. Federally qualified health clinics offer basic medical care to thousands of the uninsured at reduced rates, with no questions asked about status, but the federal government offers no insurance options for those living in the U.S. without permission.
Insurability can vary even within households, reflecting mixed immigration status among family members. Cecilia Ramirez’s mother, who does not have permission to live in the U.S., long remained uninsured, putting off treatment for uterine fibroids for years because she was worried about the cost of care.
Meanwhile, Ramirez’s children, 7-year-old Jenny and Kimberly, 3, receive insurance through Medicaid. Because they were born in the U.S., giving them citizenship, and they meet Medicaid’s eligibility standards, they are able to see primary care physicians and get other care if needed. Much of it is paid for, unlike their mother’s.
Dr. Sarah Polk, a pediatrician, provides care at the Centro Sol clinic in Baltimore to patients like Janexy Marquez-Ramirez. (Doug Kapustin for KHN)
As a foreign-born child of immigrants who entered the U.S. without permission, Ramirez’s access to health care is problematic. She applied for and received “lawfully present” status under a 2012 Obama administration policy that allowed people who arrived in the U.S. before age 16 and are now under age 35 to work and study in the U.S. without fearing deportation. Some 665,000 others have also received such status nationwide, according to figures from the Department of Homeland Security. But they were also excluded from gaining health insurance under the Affordable Care Act by a related policy of the Department of Health and Human Services. Some states, including California and New York, have softened their standards and enrolled some people here illegally in Medicaid. But nationally, most remain without coverage.
To help people like Ramirez and other low-income people without permission to live here, several institutions in East Baltimore have cobbled together an array of medical services outside of typical hospital settings. Baltimore City, Johns Hopkins Bayview, two federally subsidized clinics and one charity-run clinic offer bilingual interpreters, health providers who speak Spanish and, perhaps most importantly, low fees and sliding scales for care.
The Access Partnership, or TAP, a Johns Hopkins charitable program, offers diagnostic tests and visits to specialists for very low fees, usually no more than $20. The program serves people who lack insurance, make 200 percent or less of the federal poverty level and have been local residents for six months. More than 90 percent are Hispanic, and none are asked if they are living in the U.S. illegally, said Barbara Cook, the group’s medical director.
Cecilia Ramirez’s mother got diagnostic tests and subsequent surgery a little over a year ago to remove her uterus with help from TAP. Nonetheless, Ramirez wonders if the outcome would have been better if she had gotten help earlier.
“If she had had insurance, she might have sought out care, instead of having to wait so long that they had to remove part of her body,” she said.
The Annie E. Casey Foundation supports KHN’s coverage of health disparities in East Baltimore.
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=632831&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>632831Maryland Seeks Federal OK To Speed Ex-Inmates’ Medicaid Access
/medicaid/maryland-seeks-federal-ok-to-speed-ex-inmates-medicaid-access/
Wed, 04 May 2016 09:00:42 +0000http://khn.org/?p=619035Seeking to slash the red tape that keeps ex-prisoners with mental illness, drug addiction and other ailments from getting health coverage, Maryland is proposing to give thousands of newly released inmates temporary Medicaid membership with few questions asked.
The measure, described as the first of its kind in the nation, would help close a gap occurring when sick inmates leave jail or prison care but have trouble getting coverage and treatment after they get out, sometimes for months, advocates say.
Maryland expanded Medicaid under the Affordable Care Act, making nearly all ex-prisoners eligible for the state and federal health insurance program for low-income people. But enrollment bottlenecks have kept Maryland and other states from signing up more than a fraction of the people leaving incarceration.
The state wants the federal government to approve a stripped-down sign-up process that would give two months of Medicaid membership to released inmates who declare basic information such as residency and citizenship status. After that they would have to fully enroll, proving identification and income eligibility.
The idea, made to the federal Department of Health and Human Services on Friday, is to reduce recidivism and expensive emergency room visits by linking ex-prisoners to mental health treatment and other community care. Details would be worked out through a process of public comments and negotiations with HHS. Maryland Gov. Larry Hogan, a Republican, supports the proposal’s “overall direction,” a spokesman said.
“We want to try to eliminate as many barriers as we can” to chronically ill released prisoners seeking care, said Shannon McMahon, deputy secretary for the Department of Health and Mental Hygiene. An estimated for Medicaid late last year but still uninsured. Many are ex-inmates, say advocates. The state expanded Medicaid in 2014 to include previously excluded, low-income adults.
Inmates have of mental illness, drug addiction, and HIV and hepatitis C infections. They generally aren’t eligible for Medicaid while locked up, but advocates see jails and prisons as the perfect place to enroll them upon release.
Maryland and other states, however, have struggled to enroll them, pointing to high jail turnover, a shortage of personnel and competing tasks such as providing emerging prisoners with transportation and shelter.
“I have a heck of a time getting them to enroll, and when I don’t get them to enroll, I can’t provide continuity of care,” said Steven Rosenberg, president of Community Oriented Correctional Health Services, a California-based nonprofit that works with ex-inmates. “Why I’m excited about [Maryland’s proposal] is that the more other states understand that this is possible and that this makes sense, the more willing they will be to join the club.”
The measure would become effective next year if approved by HHS.
More than 6,000 people leave Maryland prisons each year. Thousands more cycle in and out of jails, which typically hold people who haven’t been convicted.
But the Department of Public Safety and Correctional Services has enrolled fewer than 10 percent of released inmates in Medicaid since the expansion began, The Baltimore Sun and Kaiser Health News
Last month, a fifth of Medicaid applicants at Health Care for the Homeless, many just out of prison or jail, couldn’t be processed because of problems with identification, said Barbara DiPietro, senior director of policy for the Baltimore clinic. Often people leaving incarceration “have only a prison ID, and that prison ID does not count, ironically, as a state-issued identification card” for getting Medicaid, she said.
Enrolling ex-inmates temporarily under what’s known as presumed eligibility, she said, will ensure immediate care. The state gave no cost estimate for the measure. Expanding coverage to ex-inmates could save money by reducing expensive crisis-based health care, advocates said.
Dr. Sharon Baucom, Maryland’s prison medical director, called DHMH’s proposal “a progressive leap” toward removing barriers to coverage and care.
The application could face criticism from congressional Republicans concerned that unqualified patients could get coverage.
“Getting former prisoners re-assimilated into society is well-intentioned,” said Joe Pitts, a Pennsylvania Republican who is chairman of a House health subcommittee with HHS oversight. However, he said, “Presuming eligibility on the part of all former Maryland prisoners…may not be the wisest use of taxpayer dollars.”
Federal approval for the proposal “would be huge, to minimize the red tape that is involved to help people get medical assistance,” said Rosalyn Stewart, an associate professor at the Johns Hopkins University medical school who frequently works with ex-inmates.
“What can happen if you don’t have coverage is, there’s a delay in care that can be up to 60 days,” she said.
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=619035&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>619035Thousands Leave Maryland Prisons With Risky Health Problems But No Coverage
/medicaid/thousands-leave-maryland-prisons-with-risky-health-problems-but-no-coverage/
Mon, 25 Apr 2016 09:00:39 +0000http://khn.org/?p=616175Stacey McHoul left jail last summer with a history of heroin use and depression and only a few days of medicine to treat them. When the pills ran out she started thinking about hurting herself.
“Once the meds start coming out of my system, in the past, it’s always caused me to relapse,” she said. “I start self-medicating and trying to stop the crazy thoughts in my head.”
Jail officials gave her neither prescription refills nor a Medicaid card to pay for them, she said. Within days she was back on heroin — her preferred self-medication — and sleeping in abandoned homes around Baltimore’s run-down Sandtown-Winchester neighborhood.
Thousands of people leave incarceration every year without access to the coverage and care they’re entitled to, jeopardizing their own health and sometimes the public’s.
Advocates for ex-convicts for the Affordable Care Act’s Medicaid expansion that insurance to previously excluded single adults starting in 2014, including almost everybody released from prisons and jails.
Many former inmates are mentally ill or struggle with drug abuse, diabetes or HIV and hepatitis C infection. Most return to poor communities such as West Baltimore’s Sandtown, which exploded in violence a year ago after  Freddie Gray died from injuries sustained in police custody.
But Maryland’s prison agency, which three years ago said it was  to enroll released inmates in Medicaid, is signing up fewer than a tenth of those who leave prisons and jails every year, according to state data. Few other states that have expanded Medicaid under the health law are doing any better, specialists say.
Many of them will end up in the emergency departments if we don’t attempt to connect them to services prior to release.
Traci Kodeck
Officials of the Maryland Department of Public Safety and Correctional Services say they do the best they can with limited resources, enrolling the most severely ill in Medicaid while letting most ex-inmates fend for themselves.
“We are battling, every one of us,” to maximize coverage, said prison medical director Dr. Sharon Baucom, pointing to efforts to train sign-up specialists, get Medicaid insurance for hospitalized inmates and share information on mentally ill inmates with other agencies.
“There are handoffs that could be improved,” she said. “With the resources that we currently have, and the process that we have in place, we could do more — and we just need some more help.”
Coverage under Medicaid was seen as an unprecedented chance to transform care for ex-inmates by connecting them to treatment, reducing emergency room visits, controlling disease and putting them on a path to rehabilitation.
As many as 90 percent of people leaving prisons and jails are eligible for Medicaid in states such as Maryland that expanded the federally supported program for low-income residents under the health act, experts estimate. The law gave states the option of extending Medicaid coverage to all low-income adults under 65, not just the children, pregnant women and disabled adults who were mainly included before.
Sickest Inmates Are First In Line
Some 12,000 of Maryland’s 21,000 prison inmates are designated at any given time as chronically ill with behavioral problems, diabetes, HIV, asthma, high blood pressure and other conditions, according to prison officials. But given limited means and the already tall order of connecting emerging prisoners with transportation, shelter and employment, the system focuses on enrolling the very sickest, Baucom said.
“It’s a shame to have to make that call,” she said.
(Story continues below)
A Double Burden Of Prison And Disease
By Naema Ahmed, Marissa Laliberte, Catherine Sheffo and Daniel Trielli CAPITAL NEWS SERVICE
Areas with high incarceration rates also tend to be sicker than average, as shown by HIV and imprisonment data for Baltimore. Linking released inmates to coverage and care could improve public health in these neighborhoods, advocates say.
Sources: Justice Policy Institute, Maryland Health Services Cost Review Commission
Dr. Rosalyn Stewart saw what happened to many chronically ill ex-offenders when she ran a recently completed pilot program to enroll former inmates in Medicaid and get them treatment and shelter.
“People frequently ran out of their medications and did not have access to the care they needed,” said Stewart, an associate professor at the Johns Hopkins University medical school.
McHoul, 40, spent two short stays last year in Baltimore’s Women’s Detention Center. The first time the facility released her without Medicaid coverage. Shortly afterwards she landed in a hospital with an inflamed esophagus. She got out after a second jail stay in August without knowing the hospital had enrolled her in Medicaid between incarcerations, she said.
At neither time did she have more than two weeks’ supply of any medication, including Depakote, a mood stabilizer, she said. For some prescriptions there was less than a week’s store.
“It was whatever was left in the blister pack,” said McHoul, who’s now in a Baltimore drug treatment program. “It’s like, ‘Here’s your supply. Sign this that we gave them to you. See you later.’”
State policy is to give exiting prisoners 30 days’ worth of medicine. But a court ordered McHoul released shortly after she was arrested the second time, which didn’t give the jail enough time to prepare medications, said a corrections spokesman.
There are many Stacey McHouls.
“Maybe somebody needs prescription services and they’re not enrolled and they don’t know where to go,” said Traci Kodeck, interim CEO of HealthCare Access Maryland, a nonprofit that connects consumers to coverage and has worked with the prison system. “Absolutely it happens. Many of them will end up in the emergency departments if we don’t attempt to connect them to services prior to release.”
BALTIMORE, MD — 3/22/16 — Mark Pruitt (46) is from southwest Baltimore. He is among the men dealing with addiction, and related health issues at Powell Recovery Center in Baltimore. Photo by Doug Kapustin
Lapsed Medicaid coverage barred Mark Pruitt from entering an addiction recovery program last year after he left incarceration, he said.
Mark Pruitt, 46, was released from a Baltimore facility in October with no Medicaid card and a craving for heroin, which he said he had used before he was incarcerated for a parole violation.
He desperately wanted to enter a drug treatment program, but signing up for Medicaid to pay for it was going to take weeks — far longer than he could wait.
“I knew what I wanted. I wanted help,” he said. “I really wanted help. But it’s a struggle when you’re broke — no money, no insurance, feeling defeated. Where do you turn?”
If administrators at a Baltimore recovery facility hadn’t gotten him enrolled in Medicaid, he said, “I think I’d be dead.”
From January 2014, when the Medicaid expansion took effect, through this March, Maryland released almost 16,000 people sentenced to prison or jail, according to state data. Thousands more cycle in and out of jails each year without being convicted.
But the corrections department said it enrolled only 1,337 released inmates in Medicaid from the beginning of 2014 through late March. Another 1,158 prisoners joined Medicaid over that time when they were hospitalized. (Medicaid covers inmates if they spend 24 hours as hospital inpatients; most return to prison.)
Many ex-prisoners are enrolled only when they experience a crisis and end up in an emergency room — the kind of expensive care health officials are trying to reduce. The law requires hospitals to treat emergency cases regardless of insurance coverage. They can retroactively sign those patients for Medicaid.
‘They Don’t Want To Do The Paperwork’
Monique Wright, 35, got out of Jessup Correctional Institution last fall and began suffering acute head and neck pain caused by scoliosis, a spine curvature. Without Medicaid coverage or a doctor, she said she had to seek emergency care at Johns Hopkins Bayview Medical Center.
“It’s the paperwork” that keeps prison officials from making sure people like her have Medicaid upon release, Wright said. “They don’t want to do the paperwork. They don’t have the staff to do the paperwork.”
Advocates wonder why the corrections system is so poor at enrolling what, they often point out, is “literally a captive audience.”
“They’ve had them housed for the past 10, 15 years,” said a frustrated Andre Fisher, a case manager for ex-inmates at Druid Heights Community Development Corp., a nonprofit in West Baltimore. “What’s so hard about it?”
Teressa Jackson learned the prison system hadn’t reactivated her Medicaid eligibility when she got out last year. Jackson called the medical hotline at her Medicaid managed care organization. “They said, ‘There’s nothing we can do because the jail still has a hold on your Medicaid. We can get it lifted but it may take a couple days.’” (Doug Kapustin for KHN)
Jesse Fields is a former inmate who had trouble getting drug-addiction treatment last year. “I couldn’t get on the methadone program because I didn’t have insurance. I was pretty much just out panhandling every day. Holding up a sign, ‘Need Money for Food.’ Anything I could do to get money.” (Doug Kapustin for KHN)
John Whitaker is a former inmate who discovered his Medicaid coverage had expired when he went to the hospital recently. “That’s when the lady said, ‘You know, you’re not covered with insurance.’ I said, ‘Yeah, I’m supposed to be. I got my insurance card…’ She said, ‘No, you’re not in the system right now.’ So she came back up and she put it back through for me again.” (Doug Kapustin for KHN)
Robert Alston is a house manager at A Step Forward, a Baltimore nonprofit supporting recovering drug users. “Sometimes, you know, the system doesn’t send [ex-inmates] home with that monthly supply” of medicine. “So we have to work rapidly if we come across this.” (Doug Kapustin for KHN)
Nichole Franklin is a volunteer for A Step Forward. “You need your health insurance. That’s something you can’t play with.” (Doug Kapustin for KHN)
Travis Howell is a house manager for A Step Forward. When ex-prisoners emerge without insurance, “we have to reapply and take them through the steps. It’s really time consuming, depending on the person. Depending on the situation, it can easily be a month.” (Doug Kapustin for KHN)
Enrolling inmates in Medicaid can take weeks, prison officials said. Sometimes the card doesn’t arrive until after they’re out. Computer problems slowed sign-ups in late 2014.
One mistake made by Maryland and most other states is not considering inmates for Medicaid until their release dates approach, said Colleen Barry, a professor at the Johns Hopkins Bloomberg School of Public Health who has studied the process.
“It’s a bad way to do it because you’re getting a very small number” of enrollees by waiting, she said. A better alternative is to enroll inmates when they are booked, as , she said. Those incarcerated are generally ineligible for Medicaid, but putting them in the system when they enter makes it easier to trigger coverage when they leave, she added.
Ex-Inmates Struggle To Get Medicaid Without Help
If it’s hard for the prison system to enroll inmates, it’s even harder for the individuals to enroll themselves. Those who emerge without Medicaid face a maze of applications, bus trips, phone calls and queues if they want to sign up. Many don’t bother.
For most leaving incarceration, “it’s up to you to go there, make sure you get your health insurance,” said Jamal McCoy, 21, who was living with family in West Baltimore on home detention before he was released. “Most people don’t go. Some people take it easy when they get home.”
Those who try often find that lack of identification is the first challenge. To prevent fraud, Maryland and other states require Medicaid applicants to show verified Social Security numbers.
But jails frequently lose inmate IDs, say prisoners and enrollment officials. Those locked up for years are non-persons for much of the system, with no credit records or driver’s licenses.
That can mean delays of many weeks when released prisoners are especially vulnerable. Gaps in coverage and care of even a few days after fragile patients leave the corrections health system can make the difference between life and death.
“If you’re the diabetic that hasn’t been compliant with your medication, you need your medication now,” said Henrietta Sampson, director of treatment coordination at Powell Recovery Center, a Baltimore addiction recovery agency that works with ex-inmates. “You can’t wait two weeks because you may drop dead.”
BALTIMORE, MD — 3/22/16 — William Carter (50) is from West Baltimore. He is among the men dealing with addiction, and related health issues at Powell Recovery Center in Baltimore. Photo by Doug Kapustin
Prison officials initiated Medicaid enrollment for William Carter when he was released last year. But doctors told him the program wouldn’t cover an expensive hepatitis-C drug until the virus begins damaging his liver.
Compared to the rest of the population, ex-prisoners in Washington state were  in the first two weeks after release, according to research by Dr. Ingrid Binswanger, lead researcher for Kaiser Permanente Colorado’s Institute for Health Research. Drug overdose, cardiovascular disease, homicide and suicide were the leading causes of death.
“It’s very important to manage that transition, to make sure people have continuity of care,” she said. (Kaiser Permanente has no relationship with Kaiser Health News.)
Yet in some cases the prison system has stymied outside groups trying to arrange inmates’ coverage. Stewart’s group repeatedly sought permission — “continuously, for about three years,” she said — to meet vulnerable prisoners inside the facility to get an early start on enrollment and post-release appointments. It never happened.
Baucom blamed the problem on “competing priorities” and staff turnover.
Acceptance into Medicaid by the state isn’t the end of the story. Released inmates then must enroll in a private managed-care organization hired by Maryland to provide coverage. That can take weeks longer.
Even when insured, ex-inmates face the  experienced by other low-income Baltimoreans — or worse.
Many prison inmates are , which can cause liver damage or cancer over time. But the high cost of curing the disease has prompted Maryland’s and other Medicaid programs to to those whose livers are already compromised.
“I guess I got to wait until damage is done to my liver,” said William Carter, 50, adding that prison officials initiated Medicaid enrollment when he got out last year.
Released prisoners often have no idea that some Medicaid managed-care contractors allow them to use only certain doctors and pharmacies.
If you’re the diabetic that hasn’t been compliant with your medication, you need your medication now. You can’t wait two weeks because you may drop dead.
Henrietta Sampson
“So a patient goes to Walgreens or wherever to fill something and it’s like, ‘That’ll be $150,’” because he should have gone somewhere else, said Stewart. “They don’t understand what the problem was.”
Even checking all the right boxes sometimes isn’t enough for ex-inmates, who bear the double stigma of poverty and a criminal history.
One released prisoner got an appointment to renew his mental health prescription with a facility in Carroll County, Maryland — his home — that also accepted his Medicaid card, said Baucom. After the clinic learned he had a prison record it cancelled the visit.
“It’s not enough to have a card,” Baucom said. “You’ve got to have access.”
Neighborhoods are at risk when former inmates with chronic illness return.
“You really need to think about this as a public health issue,” said Scott Nolen, director of drug treatment programs for the Open Society Institute–Baltimore, a nonprofit that works on criminal justice policy. “There is transmission of communicable diseases that happens in prison, in confined spaces. And now those folks are coming back into communities, and we want to make sure they get health care.”
In few places is the burden greater than Sandtown-Winchester. Gray, 25, died of spinal injuries that prosecutors filing manslaughter and assault charges blamed on police who arrested him.
The Justice Policy Institute, a nonprofit, called Sandtown in Baltimore last year, estimating that is in prison.
At the same time, three West Baltimore ZIP codes including Sandtown showed the highest rates of HIV infection in Maryland in 2014, according to hospital data from the Maryland Health Services Cost Review Commission obtained and analyzed by Kaiser Health News and Capital News Service.
The corrections department could use more computers, release planners and other enrollment resources, Baucom said.
“If you do the checkoff list, we’ve checked off everything we can do,” she said, noting efforts to increase enrollment capacity and cooperate with the Maryland motor vehicle agency to get inmates state IDs.
Jesse Jannetta, a specialist at the Urban Institute in prisoner re-entry, believes Maryland’s low sign-up rate “is not unusual” in other states. A found prisons and jails nationwide had enrolled 112,520 people in Medicaid from late 2013 up to January 2015, although the authors believe the actual figure was higher.
Federal and state prisons released 636,000 people in 2014, Millions more to cycle through jails each year.
Few independent experts expect Maryland — let alone most other states — to come anywhere close to full enrollment of emerging inmates anytime soon.
“It’s fair to say we’re just at the tip of the iceberg” in prisoner enrollment, said Johns Hopkins’ Barry, a coauthor of the Health Affairs study. “Maryland is always an innovator. If Maryland is still at the cutting edge of how to do this, many areas of the country don’t have any of these types of programs in place.”
This story is a partnership with The Baltimore Sun and Capital News Service, which is run by the University of Maryland’s Philip Merrill College of Journalism. KHN reporter Shefali Luthra and CNS reporters Catherine Sheffo, Daniel Trielli, Naema Ahmed and Marissa Laliberte contributed.
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=616175&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>616175In West Baltimore, Scarce Pharmacies Leave Health Care Gaps
/public-health/in-west-baltimore-scarce-pharmacies-leave-health-care-gaps/
Mon, 25 Apr 2016 09:00:26 +0000http://khn.org/?p=616179BALTIMORE — The immense new CVS dominates the corner of Pennsylvania and West North avenues. Two smaller pharmacies nearby might both fit inside. One is Keystone Pharmacy, a block away on West North. Care One is five minutes on foot up Pennsylvania.
CVS, its front shelves crammed with brightly-packaged processed foods and household cleaning supplies, is an island of abundance for this West Baltimore neighborhood, .
It’s a contrast that shows what’s changed and what hasn’t in the past year, since Freddie Gray, a 25-year-old black man, died of injuries sustained in police custody, unleashing days of protests. The CVS, just across from the Penn-North metro stop, was on April 27, demolished and rebuilt, opening again just . Looters , though both reopened within days of the protest.
But if 2015’s protests emphasized police brutality and race relations, the absence of more stores like CVS that are easily accessible to people in impoverished, predominantly black neighborhoods underscores Baltimore’s other persistent inequities.
When the CVS was closed, 51-year-old Cornell West said he traveled to a different store, a 30-minute bus ride away. The re-opened pharmacy, where he gets insomnia medicine and cortisone cream, is 10 blocks from his house. (Doug Kapustin for KHN)
Scarcity defines life in Sandtown-Winchester, the 72-block neighborhood where Gray lived for part of his life. Its roughly 9,000 residents are underserved by primary care doctors, by supermarkets that sell healthy food and by full-service retail pharmacies where anyone can pick up a prescription, buy a bottle of aspirin and a few groceries all in the same trip. No major retail pharmacies have outlets inside Sandtown. CVS, the closest to a real grocery store, is near but outside the neighborhood, as are Keystone and Care One, which don’t offer the same variety. Total Health Care, a local community health center, operates two pharmacies on the neighborhood’s border, but they also lack the non-medical variety of a CVS or Rite Aid.
Some of Baltimore’s middle- and upper-class neighborhoods lack these conveniences too, but people there have cars to get where they need to go. Most people in Sandtown must walk or take less-reliable public transportation. That’s a significant barrier for the elderly and those with chronic illnesses. The community has one of the Maryland’s highest rates of hospitalization for .
“There’s not enough quality pharmacy in West Baltimore,” said Jennifer Joseph, director of pharmacy at Total Health Care, which has 10 clinics in Baltimore, six with pharmacies.
That shortfall means disparities in accessing health care persist, despite last year’s outcry.
“Things have returned to normal, but normal still isn’t good enough,” said Anthony Pressley, director of community resources at the Druid Heights Community Development Center. Businesses such as pharmacies and grocery stores aren’t lining up to invest in the area, he added, because they assume it isn’t worth it.
(Story continues below)
Where Pharmacies Are Scarce
In certain Baltimore neighborhoods without retail chain pharmacies — such as CVS, Walgreens and Rite Aid — many residents do not have cars to drive to areas with more stores. Two examples are Sandtown-Winchester and Druid Heights.
Source: Maryland Board of Pharmacy and Baltimore Neighborhood Indicators Alliance. Data analysis by Catherine Sheffo/Capital News Service.
CVS’ 10-month closure posed hardship for some customers. Cornell West, 51, said he took a half-hour bus ride to another CVS for insomnia medication and cortisone cream. Allen Johnson, 61, filled prescriptions at Keystone but couldn’t always get what he needed, he said, such as medications for his knees, blood pressure, cholesterol, heart and diabetes.
“That was a problem for the old people. You know what I’m saying? That was a hell of a problem,” Johnson said.
If we had as many pharmacies as we had liquor stores, it would provide us more opportunity to educate, and promote health and wellness.
Jennifer Joseph
Research suggests that low-income neighborhoods in major cities with higher black and Latino populations are likely to be underserved by pharmacies. A 2014 study in illustrated that pattern in Chicago.
West Baltimore’s shortage of exacerbates the need for pharmacists who can counsel patients about basic health issues. A pharmacist is often the first line of defense for someone with a health condition, said Natalie Eddington, dean of the University of Maryland School of Pharmacy.
“For people who can’t afford health care — they don’t know how to get something,” said Haywood McMorris, the CVS store manager. “They can come here instead of going to the doctor’s and we pretty much take care of it.”
CVS and Keystone compete for that role, but on different scales.
CVS, with 27 stores in Baltimore, is the nation’s largest retail pharmacy chain based on its 9,000 U.S. outlets. It outmatches Keystone, an independent small business, on product variety and supply plus offers better hours. CVS closes at 9 p.m. on weekdays and 6 p.m. on weekends. Keystone closes three hours earlier Monday through Saturday, and it’s closed Sunday. Neither CVS nor Keystone carries fresh produce.
Ellis Basnight, 71, says he relies on the independent Keystone Pharmacy, which is a 15-minute walk from his house. Keystone’s been in the neighborhood for decades, and was one of the stores looted in last spring’s protests. (Doug Kapustin for KHN)
Keystone patrons praise its intimate service and owner Dwayne Weaver’s generosity, sometimes giving them medications on credit when they can’t afford the co-pay.
Argin Henry, 46, shops at both. He goes to CVS for groceries, drinks and goods like toilet paper, but he fills his prescriptions at Keystone, which extends credit when he’s low on cash and delivers prescriptions to his home.
A generous credit policy and delivery service are two ways Keystone competes against its much larger neighbor. CVS is in-network for every Medicaid plan in Maryland. Seven of eight plans cover drugs bought at Keystone, Weaver said. In a week, Keystone might turn away 20 to 25 customers who are out-of-network.
“We kind of survive on servicing patients in a way that chains generally don’t,” he said.
Weaver took over the pharmacy in 1985 and it’s been at its current North Avenue location for about 30 years. CVS has been there since 1997.
Ellis Basnight, who lives a 15-minute walk from Keystone, gets his drugs for diabetes, carpal tunnel and high blood pressure there.
“I’ve been coming here for years!” said Basnight, 71. “That’s why I trust him.”
Weaver considered leaving after last year’s protests. He decided to stay put after neighborhood volunteers helped clean the mess looters left.
The new CVS contains several aisles of over-the-counter medications, a contrast to the much smaller Keystone. As a major national corporation, CVS can offer a wider array of goods than can its independent peers. (Doug Kapustin for KHN)
West Baltimore’s low-income residents do have some alternatives to retail pharmacies, including two clinics of Total Health Care. Patients there can get prescriptions right after seeing the doctor, but retail pharmacies such as CVS can sate their snack cravings too.
Willie Zuber, 50, goes to CVS four blocks from home for groceries and to get medicines for an older woman he said he looks out for. He often grabs a soda or iced tea there while he waits for her prescriptions.
Joseph, Total Health Care’s pharmacy director, said CVS and Keystone likely serve the most people in the area. But they aren’t enough, she added.
“If we had as many pharmacies as we had liquor stores, it would provide us more opportunity to educate, and promote health and wellness, as opposed to alcohol and cigarettes,” she said. “You ride down the streets and what do you see? Abandoned home, abandoned home, abandoned home and liquor store. Bringing that CVS back says a lot for the city.”
Jeremy Snow is a reporter at Capital News Service. CNS reporters Brittany Britto, Ellie Silverman, Catherine Sheffo and Daniel Trielli also contributed. CNS is run by the University of Maryland’s Philip Merrill College of Journalism.
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=616179&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>616179In Freddie Gray’s Neighborhood, The Best Medical Care Is Close But Elusive
/public-health/in-freddie-grays-neighborhood-the-best-medical-care-is-close-but-elusive/
Tue, 16 Feb 2016 10:05:06 +0000The Baltimore health system put Robert Peace back together after a car crash shattered his pelvis. Then it nearly killed him, he says.
A painful bone infection that developed after surgery and a lack of follow-up care landed him in the operating room five more times, kept him homebound for a year and left him with joint damage and a severe limp.
“It’s really hard for me to trust what doctors say,” Peace said, adding that there was little after-hospital care to try to control the infection. “They didn’t do what they were supposed to do.”
Pushed by once-unthinkable shifts in how they are reimbursed, Baltimore’s famous medical institutions say they are trying harder than ever to improve the health of their lower-income neighbors in West Baltimore.
But dozens of interviews with patients, doctors and local leaders show multiple barriers between the community and the glassy hospital towers a few blocks away.
Reporters from Kaiser Health News and the spent much of the fall in and around Sandtown-Winchester, a Baltimore neighborhood where violence flared last year after Freddie Gray was fatally injured in police custody.
Residents say they have little more confidence in the medical system intended to heal them than in the criminal justice system intended to protect them.
It’s really hard for me to trust what doctors say.
Baltimore resident Robert Peace
Even though his accident happened in 2004, Peace says he cannot view doctors and hospitals with anything less than deep suspicion.
“They almost let me die,” he said.
As with so much else, there are two Baltimores when it comes to health. One population is well off and gets the best results from elite institutions on the city’s west and east sides, the University of Maryland Medical Center and the Johns Hopkins Hospital.
The other is a poor minority that gets far less, even as it uses hospital services at higher-than-average rates. One indicator: The typical Sandtown resident lives a decade less than the average American.
“They come in with a great service, but they don’t have relationships with people in the community,” said Louis Wilson, senior pastor of New Song Community Church in Sandtown, a small wedge of . “They want the people in the community to come in and respect them, but they don’t respect the people in the community. It does not work. It just doesn’t.”
The gap is more than the cultural distance between lower-income African-Americans and the wealthier practitioners, often of other ethnicities, who treat them, although that’s a part, Wilson said. It’s about insurance that is still unstable, confusing and perceived as expensive despite the health law’s recent expansion of Medicaid for low-income patients.
It’s about a system that still treats too many residents in the most expensive way possible — in crisis visits to the emergency room — rather than keeping people healthy in the community. It’s about having too few primary-care doctors addressing everyday needs to change that.
It’s about inadequate transportation to get to appointments and jail stays that cut patients off from family doctors. It’s about avoiding medical institutions often seen in the same light as the justice system that held Freddie Gray when he died: as biased, haughty and dangerous.
‘I Lost Two Aunts In That Hospital’
“When you walk into a hospital, it’s like walking into a courtroom,” said William Honablew Jr., who volunteers at LIGHT Health and Wellness, a nonprofit whose community services include helping those with HIV and other chronic illness navigate the system. “You know who’s in charge, and you know who’s not.”
Many in Sandtown have heard of Henrietta Lacks, an African-American woman whose tissue was used without permission by Johns Hopkins Hospital in the 1950s to establish a line of experimental cells. For years Baltimore blacks associated Hopkins, on the city’s east side, with the who supposedly kidnapped black children for medical experiments, residents and community leaders say.
When you walk into a hospital, it’s like walking into a courtroom. You know who’s in charge, and you know who’s not.
William Honablew Jr.
Bon Secours Baltimore Health System, Catholic, nonprofit and the nearest inpatient provider to Sandtown, has reduced potentially deadly, in-hospital hazards such as pneumonia and blood and urinary tract infections in recent years. Adjusted for illness severity, its death rates for Medicare patients with major conditions such as heart failure and stroke are little different from national scores.
But to the frustration of hospital officials who say they deserve better, Bon Secours is still known across West Baltimore as “Bon Se-Killer.”
“I lost two aunts in that hospital, an uncle and two cousins. Five people,” said Arnold Watts, 60, in a grim accounting matched, unprompted, by several other residents interviewed.
The years old, according to the Baltimore City Health Department — .
Detailed data from the Maryland agency that regulates hospital prices, seldom seen by the public, illustrate why.
Residents of the ZIP code including Sandtown accounted for the city’s second- of diabetes-related hospital cases in 2011, the second-highest rate of psychiatric cases, the sixth-highest rate of heart and circulatory cases and the second-highest rate of injury and poisoning cases. Asthma, HIV infection and drug use are common.
born in Sandtown in 2013 were underweight — the highest percentage in any of Baltimore’s 55 neighborhoods. The share of Sandtown mothers getting early prenatal care fell by 25 percentage points in 2013 from the year before.
Dr. Jay Perman is a pediatric gastroenterologist who is president of the University of Maryland, Baltimore, which shares its downtown campus with the University of Maryland Medical Center. Perman, who says the school has a critical role to play in fighting poverty, looks out of his fourteenth-floor, paneled office across a boulevard that marks the beginning of Baltimore’s poor west side.
“Why,” he asks, “in the midst of this extraordinary health care enterprise that is present in Baltimore, with all this expertise, are we sitting here on this side of Martin Luther King (Blvd.) and on the west side of Martin Luther King (Blvd.) you have some of the most disappointing life expectancies that one could imagine?”
Two miles away, residents such as David Johnson start to provide an answer. Johnson, 52, sits in the nave of First Mount Calvary Baptist Church, waiting for food-bank vegetables and talking about being newly out of jail, lacking identification and trying to qualify for Medicaid.
Police arrested Freddie Gray, 25, five blocks from the church last April, allegedly for carrying an illegal switchblade. He died of spinal injuries that prosecutors filing manslaughter charges blamed on police.
Western District police station, where officers removed Gray’s unconscious body from a prisoner van and protesters surged a week later, is a block south.
Pallbearers carry the casket of Freddie Gray to the hearse after his funeral service at New Shiloh Baptist April 27, 2015 in Baltimore. Gray, 25, was arrested for possessing a switchblade knife April 12, 2015 on Baltimore’s west side. According to his attorney, Gray died a week later in the hospital from a severe spinal cord injury he received while in police custody. (Drew Angerer/Getty Images)
Demonstrators face off with Baltimore police as a CVS pharmacy burns at the corner of Pennsylvania and North avenues during violent protests following the funeral of Freddie Gray. (Chip Somodevilla/Getty Images)
A protester walks through tear gas as police enforce a mandatory, citywide curfew on April 28, 2015. (Andrew Burton/Getty Images)
Protesters march on the street from City Hall on May 2, 2015, a day after Baltimore authorities released a report on the death of Freddie Gray. Marilyn Mosby, Baltimore City state’s attorney, ruled the death of Freddie Gray a homicide and that criminal charges would be filed against six Baltimore City Police officers. (Patrick Smith/Getty Images)
A protester holds a sign at the site of the April riots after the mistrial in the trial of Baltimore police Officer William G. Porter on Dec. 16, 2015. The judge declared a mistrial on third day of deliberations in Porter’s trial, which was the first of six trials of police officers involved in the death of Freddie Gray. (Mark Wilson/Getty Images)
A tribute to Freddie Gray marks the site near his arrest in West Baltimore. (Iman Smith/Capital News Service)
Months To Qualify For Medicaid
“I think I have diabetes,” said Johnson. “I know I have high blood pressure. I know that. I get dizzy a lot, especially when I wake up in the morning. I need to see a doctor.”
But he can’t. Baltimore jail authorities lost his identification cards, he said, before releasing him in October from an 11-month stay related to a drug arrest. He spent weeks reapplying for a Motor Vehicle Administration identification card, which social workers said he needed to qualify for Medicaid.
“You need ID to get ID, you know?” he joked. Nobody told him he could use incarceration credentials to qualify.
Medicaid’s expansion to include low-income adults was seen as an unprecedented opportunity to cover former inmates such as Johnson as they rejoin the community. (Inmates are not usually eligible while incarcerated.)
But limited administrative resources for release planning means sign-ups are often limited to the most severely ill, said Lena Hershkovitz, a vice president with HealthCare Access Maryland, a nonprofit working to increase enrollment.
“I know for a fact that he’s not unusual,” she said of Johnson. “I would say the majority of people leaving the prison or detention system are leaving without Medicaid.”
Last year the University of Maryland Medical Center found hepatitis C was causing potentially life-threatening damage to Antonio Davis’ liver, said Janet Gripshover, a nurse practitioner at the Baltimore hospital. Hepatitis C can also cause liver cancer.
Davis’ Medicaid plan, run by UnitedHealthcare, thrice denied doctors’ prescriptions for Harvoni, a new drug that can cure hepatitis C with no side effects but costs up to $90,000 for a full treatment, documents show. Davis, 58, was ineligible because he tested positive for illegal drugs or alcohol, United said in two letters to him.
“I’ve been off drugs and alcohol for six years,” he said, although he acknowledges drugs are probably how he got the virus long ago. “I don’t even drink near beer” — nonalcoholic beer.
Only by switching to a different Medicaid plan, run by Amerigroup, was he approved for Harvoni. Like many states, Maryland contracts with private insurers such as Amerigroup and United to provide Medicaid coverage.
Gripshover and other professionals acknowledge the drug’s high cost but say it saves lives and can save equally large expenses for treating cirrhosis and cancer. “There are no data” to support withholding Harvoni or other treatment from those who use illegal drugs, according to of liver-disease professionals. United declined to comment on his case.
Communication barriers and “poor customer service” are also barriers to care in West Baltimore, according to a , a Boston consultant hired by an association of community health centers.
William Ferebee, 66, has obstructive lung disease and a stent implanted after a 2001 heart attack. He avoids doctors at a University of Maryland Medical Center clinic because “they don’t even really come look at me,” he said. Instead, they give orders to a nurse or resident, “and then he comes in and says, ‘OK, here’s what we’re going to do.’”
A doctor at a nearby, independent clinic “is a sweetheart,” he said. “But it’s so hard to get an appointment.”
Distrust of the system often ensures there’s no communication at all.
Deborah Stevenson, 57, limps so badly with a damaged knee that sometimes people think she’s drunk. She believes she needs a knee replacement, “but I’m scared to get it,” she said. Her orthopedist “wouldn’t answer my questions and deal with me like a patient,” she said.
Even though she doesn’t have diabetes and her leg is otherwise healthy, her son speculated doctors might cut it off.
“I’m handicapped now,” she said. “I don’t want to be crippled.”
Fear of legal consequences also keeps people away from the health system. Some men worry doctors will report their undocumented address to social services, which they believe could reduce aid for female partners who live with them, said Wilson, the New Song pastor.
Medical privacy laws to help law enforcement officials trace suspects and fugitives. Residents subject to outstanding warrants fear they’ll be arrested if they seek care.
“Some people got a case out there — they’re not going to the health clinic,” Wilson said. “They’re going to die without giving up their information.”
Even when patients get access, care is disrupted by physician turnover, poor follow-up or insurance companies’ changing medical networks.
“The system is fragmented,” said Debbie Rock, who has run LIGHT Health and Wellness, on Sandtown’s western edge, since the 1990s. “I think that people need to go back and talk to each other. I think the doctors and the health insurance companies need to sit down and listen to each other.”
One homeless West Baltimore patient left an oral surgeon’s office with a wired jaw and no way to pay for the liquid nutrition he needed to feed himself, said Carol Marsiglia, senior vice president at the Coordinating Center, a nonprofit consulting organization that is working to reduce readmissions and emergency visits in the neighborhood.
A home-oxygen company wouldn’t serve a discharged lung patient because he had a $27 balance, she said. A hospital directed two home-health companies to teach a patient how to deal with a new colostomy bag; neither showed up. The Coordinating Center fixed the breakdowns.
Poverty makes Sandtown’s health worse. Many say poverty causes Sandtown’s poor health.
Four Liquor Stores And Three Sub Shops
Many residents hold jobs in government or manufacturing, run churches or collect pensions from the military or Social Security. Even so, the median Sandtown household
Roofs leak. Mold and mildew grow. Baltimore Gas and Electric cuts off energy to Sandtown households for nonpayment at it does in the rest of the city. Lead paint violations like the kind that are nearly four times higher in Sandtown than in Baltimore as a whole.
Drug and alcohol use are common. Diets are often poor. Many lack cars and the nearest supermarket is more than a mile away from the church.
“If we walk around this block, we’ll pass four liquor stores and three sub shops,” said Derrick DeWitt, pastor of First Mount Calvary, on Fulton Avenue.
Even small co-payments required by many health plans dissuade low-income West Baltimore residents from seeking care, the John Snow report found. Some constantly switch doctors to find the lowest price, leading to “disjointed services” and potential harm if information falls in the cracks, it found.
“I change doctors like I change underwear,” said Eddie Reaves, 64, who tries to find practices that won’t charge him copays as little as $12 or $15. His income is $1,170 a month, he said. In 2014, he added, “I must have seen a good total of about 10 doctors.”
Reaves has diabetes and high-blood pressure. He’s on Medicare because of a disability. He has applied twice to Medicaid since the health law expanded coverage two years ago. That would improve his benefits. But he never received the paperwork, he said.
The best care he ever received, Reaves said, was when he didn’t need any insurance card — when he was homeless.
“I change doctors like I change underwear sometimes” to avoid co-payments as little as $12 or $15, said Eddie Reaves, a diabetic with high blood pressure. Capital News Service photo by Iman Smith.
Health Care for the Homeless, a nonprofit a couple miles east of Sandtown, delivers comprehensive services to the homeless without regard for ability to pay.
“Didn’t have no bills,” Reaves said of the clinic when he used it a few years ago. “Your medicine they helped pay for. They did a lot for you. You could get your teeth done and everything. It was just great, man.”
The rest of the medical system is so unsatisfactory by comparison that low-income Baltimoreans sometimes claim to be homeless when they’re not, just to use the clinic, he said.
What happened after a 2004 car accident that broke Robert Peace’s pelvis is a glaring example of what many say is the kind of medicine that has been practiced too long in West Baltimore and what many say they are working to change.
Emergency surgery at UMMC fixed the fracture. But Peace developed a persistent bone infection. He received little or no follow-up care, he said, getting treatment only when the infection surged out of control and required repeated, expensive surgeries.
“The pain would be so intense — it’s like, wracking my body. I would literally sit there and shake,” he said. “That’s when I would know I had to go to the hospital, because I knew the infection was back.”
He said he required five more surgeries over a year and a half — the kind of return trips to the hospital, or “readmissions,” that the health industry and the Affordable Care Act of 2010 are trying to reduce by promoting coordination between hospitals and community doctors.
Robert Peace, outside the home of his brother in Northeast Baltimore on Jan. 15, 2016. (Doug Kapustin for KHN)
“I’m blaming it on the follow-up,” said Peace, 58. “They knew the infection wasn’t going away, but the only time they would really tend to it was when I was in the hospital.”
Today Peace walks with a cane and a pronounced limp.
It’s a story that’s still too common in West Baltimore, said Antoine Bennett, a lifelong Sandtown resident and an elder at New Song Community Church.
“We’ve got a joke here, but it’s a serious joke,” he said. “If they ain’t medicating, they’re amputating or operating. But what’s missing is the care. Primary care.”
When asked about Peace’s case, UMMC spokesman Michael Schwartzberg said, “Much has changed in the Maryland hospital environment” since his surgeries. Improvements include new emphasis on preventing readmissions and “significant investment” in care coordinators and other post-discharge management, he said.
Keeping People Healthy And Out Of The Hospital
By many accounts, hospitals, doctors, health plans and governments in Annapolis, Maryland’s capital, and Washington are making unprecedented efforts to bridge the medical divide with Sandtown and the rest of low-income Baltimore.
The grand idea is to save money and simultaneously improve lives by keeping people healthier in the community instead of letting them become ill enough to land in the hospital.
In October Bon Secours that it intends to turn into a primary care and wellness center. UMMC and Bon Secours are working with “transition coaches” from the Coordinating Center to make sure people leaving the hospitals take medicine and schedule follow-up appointments. UMMC’s transition clinic serves hundreds of recently discharged patients.
Maryland is developing one of the most advanced electronic networks for letting medical providers collaborate by sharing patient records. Health Care for the Homeless in Bon Secours.
Dr. Samuel Ross, Bon Secours’ CEO, talks about working more closely with the churches and continuing to improve the hospital’s outcomes and reputation.
BALTIMORE, MD — 2/12/16 — Dr. Samuel Ross, CEO of Bon Secures Hospital in Baltimore, Maryland. Photo by Doug Kapustin
“No, it’s not solved,” he said. “We need to keep doing what we’re doing, and understand that some of this is a person at a time. There is no wholesale campaign or branding message that’s going to cause people to say, ‘You’re wonderful.’”
In 2012 Maryland’s legislature created “health enterprise zones” to increase the supply of primary caregivers in West Baltimore and other underserved areas. UMMC puts emergency room patients in touch with a primary care doctor if they don’t have one.
In September hospitals proposed taxing insurance companies, employers and other payers so they could hire up to 1,000 caregivers directly from West Baltimore and other low-income communities with poor health results.
The Baltimore health department is pressing hospitals to collaborate on high-risk patients and is building ties with lower-income neighborhoods by hiring residents, said Dr. Leana Wen, the city’s health commissioner.
Baltimore’s B’more for Healthy Babies program has the city’s African-American infant mortality rate by nearly a third , to 12.8 per thousand births. But that’s still a fifth higher than the African-American rate for all of Maryland.
University of Maryland Medical Center has for high schoolers interested in health careers. The University of Maryland, Baltimore, got a to increase the number of African-Americans in health care jobs.
More and more professionals echo UMB’s Perman, who said a medical professional’s duty to patients does not end at the hospital or clinic door.
“As a profession, as an industry, we have not sufficiently appreciated, let alone done something about, the impact of social determinants” such as poverty, poor housing, lack of food choices and low education, he said. “Guys like me and gals like me can easily say, ‘I made the correct diagnosis. I wrote a proper prescription. I’m done.’ What I say to my students is, if you think you’re done — if ‘done’ means the patient is going to get better — you’re fooling yourself.”
Maryland’s ambitious overhaul of hospital reimbursement, authorized by the health law, is supposed to back that philosophy with powerful incentives. Starting in 2014, hospitals have been assigned annual budgets for all government and private payers, instead of being paid per admission or treatment.
The idea is to boost their motivation to contain costs by delivering preventive, community care — to pay them for keeping people out of the hospital. Hospitals are also getting penalized for excessive readmissions and preventable harm such as infections and accidental punctures.
“It’s a daunting task… when we talk about joblessness and poor nutrition and violence in the neighborhoods,” said Dr. Walter Ettinger, chief medical officer of the University of Maryland Medical System. “But we all feel driven by our mission to serve our communities in a better way, and now the finances are aligned to do that.”
Poor people, however, know that between ambitions and accomplishments is a chasm of disappointment.
In the face of wider primary-care shortages and the difficulty for doctors to make a living in low-income neighborhoods, the zone fell far short of its original goal of to West Baltimore.
“Some of the goals and objectives across almost all of the zones were a bit ambitious,” said Maura Dwyer, a senior policy advisor for the Maryland Department of Health and Mental Hygiene.
In 2014 People’s Community Health Center in Baltimore and later entered bankruptcy proceedings, demonstrating the difficulty.
Total Health Care operates several federally qualified health centers in Baltimore. (Iman Smith/Capital News Service)
Officials at Total Health Care, a federally supported nonprofit with several primary-care clinics near Sandtown, say they are proud of their service to West Baltimore.
“We want to bring the standard health in this neighborhood up to national standards,” Dr. Marcia Cort, Total’s chief medical officer, told students from the Merrill College. “We don’t want it to be the neighborhood and area [where] life expectancy is low and people are dying from preventable things.”
Still, she said, “Baltimore City is in a health crisis.”
Readmission rates for Bon Secours were still in 2014, although the Coordinating Center’s transition coaches helped reduce them by 14 percent from the year before.
Readmissions for UMMC’s midtown campus were second highest statewide after declining 5 percent, also with work by transition coaches. At UMMC’s downtown campus, readmissions were fifth highest in the state and declined 2 percent.
But state financing to pay for the transition coaches expires at the end of March. The Coordinating Center is optimistic it will be renewed but nothing is set, Marsiglia said.
In 2014 only that they understood their care after they left the hospital. For UMMC patients the figure was 51 percent.
Many resent that it took this long for the industry to try the very solutions — improving primary care, giving communities resources to help themselves — that residents of neighborhoods like Sandtown have been advocating for years.
“Unfortunately the hospitals didn’t hear us,” said Diane Bell-McKoy, CEO of Associated Black Charities, a Maryland nonprofit. “As a person of color giving that information — most people think we don’t know what we’re talking about.”
Distrust of the system, still more widespread than medical officials imagine, is passing to a new generation, residents say.
“It’s a culture that has come about over time, because younger people have seen or feel like their parents and their grandparents didn’t get the best medical treatment when they went to the hospital,” said First Mount Calvary’s DeWitt. “So they have this why-go attitude.”
Derrick DeWitt is the pastor of First Mount Calvary on Fulton Avenue in Sandtown.
On Dec. 9, Maryland regulators made three months earlier to create hospital jobs in poorer neighborhoods.
Other initiatives do little to address the low incomes and unemployment linked to Sandtown’s poor health. Nor do they simplify the shifting maze of private and government insurance plans and hospital and doctor networks that patients must navigate to get care.
One example: Nearly 2,000 low-income Medicaid members, including many in Sandtown and nearby, had to change coverage in August or get new doctors because United dropped University of Maryland Faculty Physicians from its Medicaid network in a contract dispute, said Shannon McMahon, deputy secretary of the Maryland Department of Health and Mental Hygiene.
United “had thorough continuity of care measures in place before the contract ended to ensure ongoing care was not disrupted,” said company spokesman Ben Goldstein.
For many residents, enrolling in a plan is too complicated and time-consuming, requiring time off from work to get coverage they don’t understand and can’t afford, said LIGHT Health’s Rock. In some ways the health law and its new coverage rules have made things more complex, she said.
“As the landscape is changing, people really just don’t know what to do,” she said. “They sit you down with somebody that’s supposed to help you fill [an insurance application] out, which is like a Charlie Brown episode. Once you start on the second page it’s like ‘Wah, wah, wah.’ You don’t hear nothing else. You walk out and it’s like, ‘What happened?’”
David Johnson, who was concerned about his blood pressure, dizziness and possible diabetes, joined Medicaid in December. It took two months, three trips to the motor vehicle bureau to get a new ID and two trips to social services to enroll.
An still hadn’t signed up for Medicaid as of October. As of early February, Eddie Reaves, the diabetic who gave up applying after his second attempt, was still among them.
This story is part of a reporting partnership between and University of Maryland College Park’s , which operates Capital News Service. KHN and students from the school are examining how Baltimore’s nationally respected health system serves the community where violence flared in April after Freddie Gray was fatally injured in police custody. The project is continuing. To see all the students’ work go to the .
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=600143&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>600143Video: Baltimore Hospitals Work To Repair Frayed Trust In Black Communities
/public-health/video-health-problems-fester-in-freddie-grays-neighborhood/
Tue, 16 Feb 2016 10:00:53 +0000http://khn.org/?p=599801In a city renowned for medical schools and research, there’s a striking contrast in the dismal health and life expectancy in some Baltimore neighborhoods. There’s a deep distrust of the medical system among many African-American residents, dating back to the 1800s. Kaiser Health News’ Sarah Varney reports on efforts to repair the relationship, as part of a collaboration with .
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=599801&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>599801Baltimore's Other Divide Archives - Â鶹ŮÓÅ Health News
/series/baltimore-other-divide/
Â鶹ŮÓÅ Health News produces in-depth journalism on health issues and is a core operating program of Â鶹ŮÓÅ.Thu, 16 Apr 2026 04:09:16 +0000en-US
hourly
1 https://wordpress.org/?v=6.8.5/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=32Baltimore's Other Divide Archives - Â鶹ŮÓÅ Health News
/series/baltimore-other-divide/
3232161476233Hospitals Find Asthma Hot Spots More Profitable To Neglect Than Fix
/public-health/hospitals-find-asthma-hot-spots-more-profitable-to-neglect-than-fix/
Wed, 06 Dec 2017 10:02:35 +0000BALTIMORE — Keyonta Parnell has had asthma most of his young life, but it wasn’t until his family moved to the 140-year-old house here on Lemmon Street two years ago that he became one of the health care system’s frequent customers.
“I call 911 so much since I’ve been living here, they know my name,” said the 9-year-old’s mother, Darlene Summerville, who calls the emergency medical system her “best friend.”
Summerville and her family live in the worst asthma hot spot in Baltimore: ZIP code 21223, where decrepit houses, rodents and bugs trigger the disease and where few community doctors work to prevent asthma emergencies. One mom there wields a BB gun to keep rats from her asthmatic child.
Residents of this area visit hospitals for asthma flare-ups at more than four times the rate of people from the city’s wealthier neighborhoods, according to data analyzed by Kaiser Health News and the University of Maryland’s Capital News Service.
Baltimore paramedic crews make more asthma-related visits per capita in 21223 than anywhere else in the city, according to fire department records. It is the second-most-common ZIP code among patients hospitalized for asthma, which, when addressed properly, should never require emergency visits or hospitalization.
The supreme irony of the localized epidemic is that Keyonta’s neighborhood in southwest Baltimore is in the shadow of prestigious medical centers — Johns Hopkins, whose researchers are international experts on asthma prevention, and the University of Maryland Medical Center.
Both receive massive tax breaks in return for providing “community benefit,” a poorly defined federal requirement that they serve their neighborhoods. Under Maryland’s ambitious effort to control medical costs, both are supposed to try to improve residents’ health outside the hospital and prevent admissions.
But like hospitals across the country, the institutions have done little to address the root causes of asthma. The perverse incentives of the health care payment system have long made it far more lucrative to treat severe, dangerous asthma attacks than to prevent them.
Hopkins, UMMC and other hospitals collected $84 million over the three years ending in 2015 to treat acutely ill Baltimore asthma patients as inpatients or in emergency rooms, according to the news organizations’ analysis of statewide hospital data. Hopkins and a sister hospital received $31 million of that.
Executives at Hopkins and UMMC acknowledge that they should do more about asthma in the community but note that there are many competing problems: diabetes, drug overdoses, infant mortality and mental illness among the homeless.
Science has shown it’s relatively easy and inexpensive to reduce asthma attacks: Remove rodents, carpets, bugs, cigarette smoke and other triggers. Deploy community doctors to prescribe preventive medicine and health workers to teach patients to use it.
Ben Carson, secretary of the Department of Housing and Urban Development, who saw hundreds of asthmatic children from low-income Baltimore during his decades as a Hopkins neurosurgeon, said that the research on asthma triggers is unequivocal. “It’s the environment — the moist environments that encourage the mold, the ticks, the fleas, the mice, the roaches,” he said in an interview.
Research showing that removing household triggers reduces asthma attacks “is unequivocal,” says Ben Carson, a former Johns Hopkins neurosurgeon and now secretary of the Department of Housing and Urban Development. “The cost of not taking care of people is probably greater than the cost of taking care of them.” (Katherine Gilyard/KHN)
As the leader of HUD, he says he favors reducing asthma risks in public housing as a way of cutting expensive hospital visits. The agency is discussing ways to finance pest removal, moisture control and other remediation in places asthma patients live, a spokeswoman said.
“The cost of not taking care of people is probably greater than the cost of taking care of them” by removing triggers, Carson said, adding, “It depends on whether you take the short-term view or the long-term view.”
The Long View
Asthma is the most common childhood medical condition, with rates who often live in run-down homes, than among kids in wealthier households. The disease causes nearly in the United States a year, about and thousands of deaths annually.
That drives the total annual cost of asthma care, including medicine and office visits, .
Keyonta lives in a two-bedroom row house on the 1900 block of Lemmon Street, which some residents call the “Forgetabout Neighborhood,” about a mile from UMMC and 3 miles from Hopkins.
Reporters spent months interviewing patients and parents and visiting homes in 21223, a multiracial community where the average household income of $38,911Â is lower than in all but two other ZIP codes in Maryland.
To uncover the impact of asthma, the news organizations analyzed every Maryland inpatient and emergency room case over more than three years through a special agreement with the state commission that sets hospital rates and collects such data. The records did not include identifying personal information.
For each emergency room visit to treat Baltimore residents for asthma, according to the data, hospitals were paid $871, on average. For each inpatient case, the average revenue was $8,698. In one recent three-year period, hospitals collected $6.1 million for treating just 50 inpatients, the ones most frequently ill with asthma, each of whom visited the hospital at least 10 times.
Lemmon Street’s trash piles and vacant homes harbor rodents and insects that can set off asthma flare-ups. (Doug Kapustin for KHN)
Darlene Summerville partly blames a moldy dirt basement for triggering her children’s asthma flare-ups. (Doug Kapustin for KHN)
shows that shifting dollars from hospitals to Lemmon Street and other asthma hot spots could more than pay for itself. Half the cost of one admission — a few thousand dollars — could buy air purifiers, pest control, visits by community health workers and other measures proven to slash asthma attacks and hospital visits by frequent users.
“We love” these ideas, and “we think it’s the right thing to do,” said Patricia Brown, a senior vice president at Hopkins in charge of managed care and population health. “We know who these people are. . . . This is doable, and somebody should do it.”
But converting ideas to action hasn’t happened at Hopkins or much of anywhere else.
One of the few hospitals making a substantial effort, Children’s National Health System in Washington, D.C., has found that its good work comes at a price to its bottom line.
Children’s sends asthma patients treated in the emergency room to that teaches them and their families how to take medication properly and remove home triggers. The program, begun in the early 2000s, cut emergency room use and other unscheduled visits by those patients by 40 percent, a study showed.
While recognizing that it decreases potential revenue, hospital managers fully support the program, said Dr. Stephen Teach, the pediatrics chief who runs it.
“‘Asthma visits and admissions are down again, and it’s all your fault!’” Children’s chief executive likes to tease him, Teach said. “And half his brain is actually serious, but the other half of his brain is celebrating the fact that the health of the children of the District of Columbia is better.”
I call 911 so much since I’ve been living here, they know my name.
Darlene Summerville
The Close-Up View
Half of the 32 row houses on Summerville’s block of Lemmon Street are boarded up, occupied only by the occasional heroin user. At least 10 people on the block had asthma late last year, according to interviews with residents then.
“We have mold in our house” and a leaky roof, said Tracy Oates, 42, who lived across the street from Summerville. “That is really big trouble as far as triggering asthma.”
Two of her children have the disease. “I don’t even want to stay here,” she said. “I’m looking for a place.”
Shadawnna Fews, 30, lived with her asthmatic toddler on Stricker Street, a few blocks east. She kept a BB gun to pick off rats that doctors said can set off her son’s wheezing.
Delores Jackson, 56, who lived on Wilkens Avenue, a few blocks south of Lemmon Street, said she had been to the hospital for asthma three times in the previous month.
All three of Summerville’s kids have asthma. Before moving to Lemmon Street two years ago, she remembers, Keyonta’s asthma attacks rarely required medical attention.
But their new house contained a clinical catalog of asthma triggers.
The moldy basement has a dirt floor. Piles of garbage in nearby vacant lots draw vermin: mice, which are , along with rats. Summerville, 37, kept a census of invading insects: gnats, flies, spiders, ants, grasshoppers, “little teeny black bugs,” she laughed.
Often she smokes inside the house.
The state hospital data show that about 25 Marylanders die annually from acute asthma, their airways so constricted and blocked by mucus that they suffocate.
Keyonta missed dozens of school days last year because of his illness, staying home so often that Summerville had to quit her cooking job to care for him. Without that income, the family nearly got evicted last fall and again in January. The rent is $750.
About a third of Baltimore high school students report they have had asthma, causing frequent absences and missed learning, said Dr. Leana Wen, Baltimore’s health commissioner.
With numbers like that, West Baltimore’s primary care clinics, which treat a wide range of illnesses, as is the city health department’s asthma program, whose three employees visit homes of asthmatic children to demonstrate how to take medication and reduce triggers.
The program, which an analysis by Wen’s office showed cut asthma symptoms by 89 percent, “is chronically underfunded,” she said. “We’re serving 200 children [a year], and there are thousands that we could expand the program to.”
‘The Hospital Instead Of The Classroom’
The federal government paid for $1.3 billion in asthma-related research over the past decade, of which $205 million went to Hopkins, records show. The money supports basic science as well as many studies showing that modest investments in community care and home remediation can improve lives and save money.
“Getting health care providers to pay for home-based interventions is going to be necessary if we want to make a dent in the asthma problem,” said Patrick Breysse, a former Hopkins official, who as director of the National Center for Environmental Health at the Centers for Disease Control and Prevention is one of the country’s top public health officials.
Other factors can trigger asthma: outdoor air pollution and pollen, in particular. But eliminating home-based triggers could , one study showed.
Perhaps no better place exists to try community asthma prevention than Maryland. By guaranteeing hospitals’ revenue each year, the state’s unique rate-setting system encourages them to cut admissions with preventive care, policy authorities say.
But Hopkins, UMMC and their corporate parents, whose four main Baltimore hospitals together collect some $5 billion in revenue a year, have so far limited their community asthma prevention to small, often temporary efforts, often financed by somebody else’s money.
UMMC’s Breathmobile program, which visits Baltimore schools dispensing asthma treatment and education, depends on outside grants and could easily be expanded with the proper resources, said its medical director, Dr. Mary Bollinger. “The need is there, absolutely,” she said.
Hopkins runs “Camp Superkids,” a weeklong, sleep-away summer session for children with asthma that costs participants $400, although it awards scholarships to low-income families. It’s also conducting yet another study — testing referral to follow-up care for emergency room asthma patients, which Children’s National long ago showed was effective.
But no hospital has invested substantially in home remediation to eliminate triggers, a proven strategy supported by the HUD secretary and promoted by Green and Healthy Homes Initiative, a Baltimore nonprofit that works to reduce asthma and lead poisoning.
“We either go forward to do what has been empirically shown to work, or we continue to bury our heads in the sand and kids will continue to go to the hospital instead of the classroom,” said Ruth Ann Norton, the nonprofit’s chief executive.
Hopkins and UMMC say they do plenty to earn their community benefit tax breaks.
“It’s always a challenge to say, ‘Where do we start first?’” said Dana Farrakhan, a senior vice president at UMMC whose duties include community health improvement.
Among other initiatives, UMMC takes credit for working with city officials to sharply reduce infant mortality by working with expectant mothers. The organization’s planned outpatient center will include health workers to help people reduce home asthma triggers, Farrakhan said.
“What we do is perhaps not sufficiently focused,” Brown of Hopkins said. At the same time, “we have to have revenue,” she said. “We’re a business.”
After months of waiting, Summerville considered herself lucky to get an appointment with the city health department’s asthma program.
One of its health workers came to the house late last year. She supplied mousetraps and mattress and pillow covers to control mites and other triggers. She helped force Summerville’s landlord to fix holes in the ceiling and floor.
She urged Summerville to stop smoking inside and gave medication lessons, which uncovered that Summerville had mixed up a preventive inhaler with the medicine used for Keyonta’s flaring symptoms.
“The asthma lady taught me what I needed to know to keep them healthy,” Summerville said of her family.
That was late in 2016. Since then, Summerville said last month, she hasn’t called an ambulance.
METHODOLOGY:
Kaiser Health News and the University of Maryland’s Capital News Service obtained data held by the Maryland Health Services Cost Review Commission on every hospital inpatient and emergency room case in the state from mid-2012 to mid-2016 — some 10 million cases. The anonymized data did not include identifying personal information.
The news organizations measured asthma costs by calculating total charges for cases in which asthma was the principal diagnosis. Maryland’s hospital rate-setting system ensures that such listed charges are very close to equaling the payments collected.
To determine asthma prevalence, reporters calculated the per capita rate of hospital visits with asthma as a principal diagnosis — a method frequently used by health departments and researchers. This may exaggerate asthma prevalence in low-income ZIP codes such as 21223, because of those communities’ tendency to use hospital services at greater rates.
However, the data also point to high asthma rates in 21223 and other low-income Baltimore communities — for example, asthma prevalence within the population of all hospital patients in a ZIP code.
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=793426&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>793426Attack On Asthma: Scrubbing Homes Of Allergens May Tame Disease And Its Costs
/public-health/attack-on-asthma-scrubbing-homes-of-allergens-can-tame-disease-and-its-costs/
Wed, 06 Dec 2017 10:00:49 +0000After years of studying the causes of asthma, a pediatrician-turned-public health sleuth thinks there’s a way to substantially reduce its impact.
But the approach faces a big hurdle: getting someone to pay for it, said Dr. Elizabeth Matsui, a professor at Johns Hopkins medical school in Baltimore.
Matsui, who suffered from asthma as a child, has spent much of her career studying the link between poor housing and asthma in low-income neighborhoods. In particular, she’s looked at the effects of mouse allergens, typically found in high concentrations in urban homes.
Matsui cited a 2004 study in the New England Journal of Medicine that described measures to reduce home allergen levels and concluded that they were linked to reductions in asthma symptoms.
That research “was highly successful and impactful,” but the approach wasn’t widely adopted, Matsui said.
“So here we have this trial that was published more than 10 years ago that shows [indoor allergen control] works,” said Matsui, who did not participate in the study. “But the families who need it most can’t afford to do these things, don’t have control oftentimes over their home environment, and insurance or other payers don’t cover these things.”
Matsui has proposed new incentives for hospitals to provide home intervention, including Medicaid waivers. But, she said, scientists can’t use research money for these programs. “Delivery of community health care programs would require a different type of funding.”
As a result, doctors and scientists doubted if a plan to control home allergens would scale up, and insurers questioned whether benefits to their bottom line would justify the added cost.
“We have this enormous public health problem in that there are housing conditions that directly affect allergen exposure in this population of kids,” Matsui said. “We have dedicated individuals and groups who are trying to solve the problem. But we don’t have a system that is able to solve the problem.”
A by Matsui, published in the Journal of the American Medical Association, suggests that even without intensive professional cleaning services, families that receive some training can substantially reduce home allergens on their own.
That finding suggests health agencies should routinely offer to educate asthma-affected families in home allergen control. “There’s potentially a large benefit,” Matsui said.
In a separate study, Matsui’s group is following 200 Baltimore children to see if those in homes scrubbed of allergens need fewer treatments with rescue inhalers. If they do, that could give health insurers an incentive to pay for the approach.
There’s another incentive: Clearing the air in a child’s home may be critical in cases where medications alone don’t work. “We continue to see a lot of kids that, despite being on medication, don’t have well-controlled asthma,” Matsui said.
Asthma drugs can also have serious side effects, she said, especially at higher doses, and may suppress symptoms without halting lung damage.
Matsui’s work on asthma began while working as a pediatrician at Baltimore’s Franklin Square Hospital in 1998. As part of her job, she spent half a day each week in a school health clinic in a low-income area.
Matsui was struck by the number of kids she saw with severe asthma, she said, and set up a home health visit program to help them. But she wasn’t certain the program was working, so she consulted with experts at Hopkins.
In 2004, she earned a master’s from the Hopkins school of public health. Today, she is one of the nation’s leading asthma researchers.
Matsui said her career was shaped by her own struggle with childhood asthma. “I think that that probably played a role, consciously or unconsciously,” she said.
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=741260&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>741260Baltimore Draws 10-Year Blueprint To Cut Racial Health Disparities
/public-health/baltimore-draws-10-year-blueprint-to-cut-racial-health-disparities/
Wed, 31 Aug 2016 11:21:04 +0000http://khn.org/?p=654494Baltimore officials presented a 10-year plan Tuesday that sharply highlights the poor health status of African-Americans and aims to bring black rates of lead poisoning, heart disease, obesity, smoking and overdoses more in line with those of whites.
“We wanted to specifically call out disparities” in racial health, said Dr. Leana Wen, who became the city’s health commissioner early last year. “And we have a moonshot. Our moonshot is we want to cut health disparities by half in the next 10 years.”
Black Baltimore leaders praised Wen for putting disparities squarely in the conversation even as they acknowledged the difficulty of achieving the plan’s goals.
“It’s a big challenge. There’s no debating that,” said Diane Bell-McKoy, CEO of Associated Black Charities, a Maryland nonprofit. “She takes a step forward more so than anybody else I’ve seen because she calls it out. Most of the time we find code words for it. We don’t call it out.”
Violence last year following the death of Freddie Gray, a black man who died after being injured in police custody,  as well as its criminal justice differences, officials said. Gray’s family had won a settlement for alleged lead-paint poisoning, which is blamed for low test scores and cognitive challenges among thousands of Baltimore children.
“What happened last year with Freddie Gray put Baltimore in the national media spotlight,” said Helen Holton, a Baltimore councilwoman who represents a portion of the city’s west side. “That made people stop and take notice of what had been going on and stop treating it as business as usual.”
°Õ³ó±ðÌý, called Healthy Baltimore 2020, was  by the Baltimore Sun. Officials plan to track blood-lead levels, overdose deaths, child fatalities, healthy-food availability and other indicators year by year. It’s called Healthy Baltimore 2020 because officials have set ambitious goals to achieve before 10 years is up, Wen said.
Tentative targets include cutting youth homicides by 10 percent and disparities in obesity, smoking and heart-disease deaths by 15 percent — all by 2020.
Tactics include more programs to reduce street violence, expanded anti-smoking campaigns, more home visits for pregnant women and increased access to naloxone, which blocks the effects of heroin.
The blueprint is “an ongoing document” that will be amended with community participation and results closely scored, Wen said.
“Our community is sick of us overpromising and underdelivering,” she said.
Baltimore officials have made substantial progress in ,Ìý±ô´Ç·É±ð°ù¾±²Ô²µÌý and cutting .
But as in many other areas, Baltimore is still divided by health. Residents of Gray’s west-side neighborhood of  live 10 years less on average than Marylanders in general. Poor neighborhoods have far higher rates of heart disease, diabetes, addiction, HIV infection and other illness than more prosperous parts of the city.
Black leaders emphasized that Baltimore’s health won’t improve unless policymakers address deeper causes of illness such as poverty, unemployment and poor housing.
“It is affirming to see someone in Dr. Wen’s role address the uncomfortable truths behind health inequities,” said Debbie Rock, CEO of LIGHT Health and Wellness, which offers health and other community services on Baltimore’s west side. “This is a great platform to also address upstream factors” such as low incomes, she said.
Holton compared the health blueprint to a  alleging a pattern of excessive force and violation of constitutional rights by the Baltimore Police Department.
Both documents address racial differences and offer challenges for improvement, she said.
“You can travel 5Â miles from one neighborhood to another and it’s like you are in two different communities” in health levels, Holton said. “Freddie Gray was like the tipping point. Let’s take this and make it a teachable moment of how to be better moving forward.”
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=654494&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>654494A Young Latina In Baltimore Struggles To Keep Her Family Healthy
/public-health/a-young-latina-in-baltimore-struggles-to-keep-her-family-healthy/
Fri, 08 Jul 2016 09:00:58 +0000http://khn.org/?p=637173Mom Marlene (left) and daughter Nathaly (right) are finally insured with a special program. Younger daughter Stephanie (center) has had more access to care because she is a U.S. citizen. (Mary Wiltenburg for KHN)
Nathaly Uribe works in a busy insurance office in East Baltimore. But while she sells car and home insurance all day, she can’t afford health coverage for herself.
Uribe is a DREAMer, meaning she qualifies for the Obama administration’s “deferred action” program for people who came to this country as small children. Her mother is undocumented and her sister is a citizen.
Reporting for WYPR and Kaiser Health News, Mary Wiltenburg explores how this mix of immigration status and low income have been barriers to health care for the family.
Listen to the radio story below and click  to read more.
The Annie E. Casey Foundation supports KHN’s coverage of health disparities in East Baltimore.
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=637173&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>637173For Many In Baltimore’s Growing Latino Community, Health Care Is A Challenge
/insurance/for-many-in-baltimores-growing-latino-community-health-care-is-a-challenge/
Mon, 27 Jun 2016 09:00:49 +0000http://khn.org/?p=632831Cecilia Ramirez is worried about her weight and troubling symptoms that hint of diabetes, but she won’t seek medical help because she can’t afford it.
“I don’t go to the doctor when I’m sick — it’s too expensive,” she said.
Though she is a sales worker at an insurance agency in Highlandtown, an East Baltimore neighborhood that has seen an influx of Hispanic immigrants in recent years, Ramirez, 23, has no health insurance.
Her predicament is shared by thousands of Hispanic immigrants in East Baltimore, and millions nationally, who cannot afford regular medical services and are uninsured because they lack the benefits attached to legal U.S. residency and citizenship.
Ramirez’s parents came illegally to the U.S. from Mexico when she was 10. Her immigration status now — “lawfully present” — allows her to work and study here without fear of deportation, but she has no path to citizenship. She is ineligible for health coverage under the Affordable Care Act or any public insurance program.
(The Supreme Court’s decision last week in a related immigration case did not change this.)
Her $23,000 annual income would easily qualify her for Medicaid, but only her two young children can get it. Ramirez’s employer can’t afford to offer her private health insurance either, and even if it did, she doubts she could afford it. So, how can Ramirez deal with the hacking from her lungs?
“Vicks VapoRub,” offers her boss, David Rosario, drawing cynical laughter from Ramirez and others in the office.
Latinos, uninsured or not, face many challenges when it comes to finding medical care. Many have trouble speaking and understanding English, are poor and undereducated, or lack transportation. Others come from cultures where health care is a luxury they don’t regularly seek out.
Cecilia Ramirez and her two daughters, Jenny Rodriguez-Ramirez, 7, and Kimberly Gonzalez-Ramirez, 3. The girls qualify for Medicaid because they were born in the U.S., but their mother does not because of her immigration status. (Doug Kapustin for KHN)
But the inability of non-citizens to join affordable health plans remains the primary stumbling block separating people from Mexico, Central America and South America from care.
“What we’re seeing across the country is that the undocumented are one of the most vulnerable groups out there when it comes to insurability,” said Steven Lopez, manager of the health policy project at the National Council of La Raza, the largest Latino advocacy group in the U.S. “The opportunity to get regular health care is the key to finding greater opportunity. If you don’t have your health, you’re not going to progress in life.”
Nationwide, more than 5 million people living in the U.S. illegally are without medical coverage, with indications that most are Hispanic, according to an released in March. Nearly half of all immigrants living here without permission are uninsured, compared with 10.5 percent of U.S. citizens and roughly 15 percent of non-citizens living here legally, the report noted. Hispanic adults’ uninsured rate fell to 28 percent last year — 13 percentage points below 2013 — but remains far higher than those of non-Hispanic whites, blacks and Asians, according to released in May.
“This is the tricky part for us,” said Leana Wen, Baltimore’s health commissioner. “The Affordable Care Act excludes these individuals” who lack authorization to live in the U.S. “They fall through the cracks.”
They have done so even as Mayor Stephanie Rawlings-Blake works to draw more immigrants here in the hope they will repopulate hollowed out inner-city blocks. Latinos, who figure prominently in the mayor’s drive to recruit 10,000 new families, continue to filter into several older East Baltimore neighborhoods, including Fells Point, Greektown, Highlandtown and Patterson Park.
Baltimore’s population includes around 30,000 Latinos, up from just 9,000 15 years ago, city officials say. Medical providers and Latino advocates say that 40 to 60 percent of them live in the U.S. illegally, a range close to the Urban Institute’s national estimates.
Health is a major concern. Baltimore Latinos are twice as likely as non-Latinos to say they have poor or fair health, according to a in 2011.
There is insufficient data to make judgments about the health of the city’s Latinos or compare them to other groups. But death from cardiovascular disease and cancer were the two leading causes of death among the city’s Latinos in 2012, according to a 2014 report by the department. Unintentional injury and chronic liver disease or cirrhosis tied for the fourth leading cause of death among the city’s Latinos, but they were much less common among white and black populations, the report found.
“People can start businesses and buy homes, but they can’t get medical insurance,” said Rosario, who serves as board president for the Latino Providers Network, an organization that links Hispanics to services.
Working out of an office within Johns Hopkins Hospital’s Bayview Medical Center in Baltimore, Centro SOL social worker Flor Giusti converses with Latino patients in her office there. (Doug Kapustin for KHN)
As a result, health providers say that when they see people come into their offices or clinics, they are often in advanced stages of illness.
“Typically, we see a lot of diabetes and obesity-related diseases, like high blood pressure,” said Kathleen Page, an infectious disease specialist at Johns Hopkins Hospital and a cofounder of Centro SOL, a Bayview outreach program that treats Hispanic clients at reduced prices. Baltimore Latinos suffer higher rates of those disorders despite being younger as a group than the rest of the city’s population. Chronic infections and mental health problems such as anxiety and depression run rampant, Page added.
About 95 percent of the Hispanic patients she sees at her HIV clinic are living here illegally and lack health insurance.
Latinos’ ability to find treatment is tied directly to their immigration status.
Some people in the U.S. without documentation can receive payments for baby deliveries through Emergency Medicaid. Federally qualified health clinics offer basic medical care to thousands of the uninsured at reduced rates, with no questions asked about status, but the federal government offers no insurance options for those living in the U.S. without permission.
Insurability can vary even within households, reflecting mixed immigration status among family members. Cecilia Ramirez’s mother, who does not have permission to live in the U.S., long remained uninsured, putting off treatment for uterine fibroids for years because she was worried about the cost of care.
Meanwhile, Ramirez’s children, 7-year-old Jenny and Kimberly, 3, receive insurance through Medicaid. Because they were born in the U.S., giving them citizenship, and they meet Medicaid’s eligibility standards, they are able to see primary care physicians and get other care if needed. Much of it is paid for, unlike their mother’s.
Dr. Sarah Polk, a pediatrician, provides care at the Centro Sol clinic in Baltimore to patients like Janexy Marquez-Ramirez. (Doug Kapustin for KHN)
As a foreign-born child of immigrants who entered the U.S. without permission, Ramirez’s access to health care is problematic. She applied for and received “lawfully present” status under a 2012 Obama administration policy that allowed people who arrived in the U.S. before age 16 and are now under age 35 to work and study in the U.S. without fearing deportation. Some 665,000 others have also received such status nationwide, according to figures from the Department of Homeland Security. But they were also excluded from gaining health insurance under the Affordable Care Act by a related policy of the Department of Health and Human Services. Some states, including California and New York, have softened their standards and enrolled some people here illegally in Medicaid. But nationally, most remain without coverage.
To help people like Ramirez and other low-income people without permission to live here, several institutions in East Baltimore have cobbled together an array of medical services outside of typical hospital settings. Baltimore City, Johns Hopkins Bayview, two federally subsidized clinics and one charity-run clinic offer bilingual interpreters, health providers who speak Spanish and, perhaps most importantly, low fees and sliding scales for care.
The Access Partnership, or TAP, a Johns Hopkins charitable program, offers diagnostic tests and visits to specialists for very low fees, usually no more than $20. The program serves people who lack insurance, make 200 percent or less of the federal poverty level and have been local residents for six months. More than 90 percent are Hispanic, and none are asked if they are living in the U.S. illegally, said Barbara Cook, the group’s medical director.
Cecilia Ramirez’s mother got diagnostic tests and subsequent surgery a little over a year ago to remove her uterus with help from TAP. Nonetheless, Ramirez wonders if the outcome would have been better if she had gotten help earlier.
“If she had had insurance, she might have sought out care, instead of having to wait so long that they had to remove part of her body,” she said.
The Annie E. Casey Foundation supports KHN’s coverage of health disparities in East Baltimore.
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=632831&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>632831Maryland Seeks Federal OK To Speed Ex-Inmates’ Medicaid Access
/medicaid/maryland-seeks-federal-ok-to-speed-ex-inmates-medicaid-access/
Wed, 04 May 2016 09:00:42 +0000http://khn.org/?p=619035Seeking to slash the red tape that keeps ex-prisoners with mental illness, drug addiction and other ailments from getting health coverage, Maryland is proposing to give thousands of newly released inmates temporary Medicaid membership with few questions asked.
The measure, described as the first of its kind in the nation, would help close a gap occurring when sick inmates leave jail or prison care but have trouble getting coverage and treatment after they get out, sometimes for months, advocates say.
Maryland expanded Medicaid under the Affordable Care Act, making nearly all ex-prisoners eligible for the state and federal health insurance program for low-income people. But enrollment bottlenecks have kept Maryland and other states from signing up more than a fraction of the people leaving incarceration.
The state wants the federal government to approve a stripped-down sign-up process that would give two months of Medicaid membership to released inmates who declare basic information such as residency and citizenship status. After that they would have to fully enroll, proving identification and income eligibility.
The idea, made to the federal Department of Health and Human Services on Friday, is to reduce recidivism and expensive emergency room visits by linking ex-prisoners to mental health treatment and other community care. Details would be worked out through a process of public comments and negotiations with HHS. Maryland Gov. Larry Hogan, a Republican, supports the proposal’s “overall direction,” a spokesman said.
“We want to try to eliminate as many barriers as we can” to chronically ill released prisoners seeking care, said Shannon McMahon, deputy secretary for the Department of Health and Mental Hygiene. An estimated for Medicaid late last year but still uninsured. Many are ex-inmates, say advocates. The state expanded Medicaid in 2014 to include previously excluded, low-income adults.
Inmates have of mental illness, drug addiction, and HIV and hepatitis C infections. They generally aren’t eligible for Medicaid while locked up, but advocates see jails and prisons as the perfect place to enroll them upon release.
Maryland and other states, however, have struggled to enroll them, pointing to high jail turnover, a shortage of personnel and competing tasks such as providing emerging prisoners with transportation and shelter.
“I have a heck of a time getting them to enroll, and when I don’t get them to enroll, I can’t provide continuity of care,” said Steven Rosenberg, president of Community Oriented Correctional Health Services, a California-based nonprofit that works with ex-inmates. “Why I’m excited about [Maryland’s proposal] is that the more other states understand that this is possible and that this makes sense, the more willing they will be to join the club.”
The measure would become effective next year if approved by HHS.
More than 6,000 people leave Maryland prisons each year. Thousands more cycle in and out of jails, which typically hold people who haven’t been convicted.
But the Department of Public Safety and Correctional Services has enrolled fewer than 10 percent of released inmates in Medicaid since the expansion began, The Baltimore Sun and Kaiser Health News
Last month, a fifth of Medicaid applicants at Health Care for the Homeless, many just out of prison or jail, couldn’t be processed because of problems with identification, said Barbara DiPietro, senior director of policy for the Baltimore clinic. Often people leaving incarceration “have only a prison ID, and that prison ID does not count, ironically, as a state-issued identification card” for getting Medicaid, she said.
Enrolling ex-inmates temporarily under what’s known as presumed eligibility, she said, will ensure immediate care. The state gave no cost estimate for the measure. Expanding coverage to ex-inmates could save money by reducing expensive crisis-based health care, advocates said.
Dr. Sharon Baucom, Maryland’s prison medical director, called DHMH’s proposal “a progressive leap” toward removing barriers to coverage and care.
The application could face criticism from congressional Republicans concerned that unqualified patients could get coverage.
“Getting former prisoners re-assimilated into society is well-intentioned,” said Joe Pitts, a Pennsylvania Republican who is chairman of a House health subcommittee with HHS oversight. However, he said, “Presuming eligibility on the part of all former Maryland prisoners…may not be the wisest use of taxpayer dollars.”
Federal approval for the proposal “would be huge, to minimize the red tape that is involved to help people get medical assistance,” said Rosalyn Stewart, an associate professor at the Johns Hopkins University medical school who frequently works with ex-inmates.
“What can happen if you don’t have coverage is, there’s a delay in care that can be up to 60 days,” she said.
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=619035&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>619035Thousands Leave Maryland Prisons With Risky Health Problems But No Coverage
/medicaid/thousands-leave-maryland-prisons-with-risky-health-problems-but-no-coverage/
Mon, 25 Apr 2016 09:00:39 +0000http://khn.org/?p=616175Stacey McHoul left jail last summer with a history of heroin use and depression and only a few days of medicine to treat them. When the pills ran out she started thinking about hurting herself.
“Once the meds start coming out of my system, in the past, it’s always caused me to relapse,” she said. “I start self-medicating and trying to stop the crazy thoughts in my head.”
Jail officials gave her neither prescription refills nor a Medicaid card to pay for them, she said. Within days she was back on heroin — her preferred self-medication — and sleeping in abandoned homes around Baltimore’s run-down Sandtown-Winchester neighborhood.
Thousands of people leave incarceration every year without access to the coverage and care they’re entitled to, jeopardizing their own health and sometimes the public’s.
Advocates for ex-convicts for the Affordable Care Act’s Medicaid expansion that insurance to previously excluded single adults starting in 2014, including almost everybody released from prisons and jails.
Many former inmates are mentally ill or struggle with drug abuse, diabetes or HIV and hepatitis C infection. Most return to poor communities such as West Baltimore’s Sandtown, which exploded in violence a year ago after  Freddie Gray died from injuries sustained in police custody.
But Maryland’s prison agency, which three years ago said it was  to enroll released inmates in Medicaid, is signing up fewer than a tenth of those who leave prisons and jails every year, according to state data. Few other states that have expanded Medicaid under the health law are doing any better, specialists say.
Many of them will end up in the emergency departments if we don’t attempt to connect them to services prior to release.
Traci Kodeck
Officials of the Maryland Department of Public Safety and Correctional Services say they do the best they can with limited resources, enrolling the most severely ill in Medicaid while letting most ex-inmates fend for themselves.
“We are battling, every one of us,” to maximize coverage, said prison medical director Dr. Sharon Baucom, pointing to efforts to train sign-up specialists, get Medicaid insurance for hospitalized inmates and share information on mentally ill inmates with other agencies.
“There are handoffs that could be improved,” she said. “With the resources that we currently have, and the process that we have in place, we could do more — and we just need some more help.”
Coverage under Medicaid was seen as an unprecedented chance to transform care for ex-inmates by connecting them to treatment, reducing emergency room visits, controlling disease and putting them on a path to rehabilitation.
As many as 90 percent of people leaving prisons and jails are eligible for Medicaid in states such as Maryland that expanded the federally supported program for low-income residents under the health act, experts estimate. The law gave states the option of extending Medicaid coverage to all low-income adults under 65, not just the children, pregnant women and disabled adults who were mainly included before.
Sickest Inmates Are First In Line
Some 12,000 of Maryland’s 21,000 prison inmates are designated at any given time as chronically ill with behavioral problems, diabetes, HIV, asthma, high blood pressure and other conditions, according to prison officials. But given limited means and the already tall order of connecting emerging prisoners with transportation, shelter and employment, the system focuses on enrolling the very sickest, Baucom said.
“It’s a shame to have to make that call,” she said.
(Story continues below)
A Double Burden Of Prison And Disease
By Naema Ahmed, Marissa Laliberte, Catherine Sheffo and Daniel Trielli CAPITAL NEWS SERVICE
Areas with high incarceration rates also tend to be sicker than average, as shown by HIV and imprisonment data for Baltimore. Linking released inmates to coverage and care could improve public health in these neighborhoods, advocates say.
Sources: Justice Policy Institute, Maryland Health Services Cost Review Commission
Dr. Rosalyn Stewart saw what happened to many chronically ill ex-offenders when she ran a recently completed pilot program to enroll former inmates in Medicaid and get them treatment and shelter.
“People frequently ran out of their medications and did not have access to the care they needed,” said Stewart, an associate professor at the Johns Hopkins University medical school.
McHoul, 40, spent two short stays last year in Baltimore’s Women’s Detention Center. The first time the facility released her without Medicaid coverage. Shortly afterwards she landed in a hospital with an inflamed esophagus. She got out after a second jail stay in August without knowing the hospital had enrolled her in Medicaid between incarcerations, she said.
At neither time did she have more than two weeks’ supply of any medication, including Depakote, a mood stabilizer, she said. For some prescriptions there was less than a week’s store.
“It was whatever was left in the blister pack,” said McHoul, who’s now in a Baltimore drug treatment program. “It’s like, ‘Here’s your supply. Sign this that we gave them to you. See you later.’”
State policy is to give exiting prisoners 30 days’ worth of medicine. But a court ordered McHoul released shortly after she was arrested the second time, which didn’t give the jail enough time to prepare medications, said a corrections spokesman.
There are many Stacey McHouls.
“Maybe somebody needs prescription services and they’re not enrolled and they don’t know where to go,” said Traci Kodeck, interim CEO of HealthCare Access Maryland, a nonprofit that connects consumers to coverage and has worked with the prison system. “Absolutely it happens. Many of them will end up in the emergency departments if we don’t attempt to connect them to services prior to release.”
BALTIMORE, MD — 3/22/16 — Mark Pruitt (46) is from southwest Baltimore. He is among the men dealing with addiction, and related health issues at Powell Recovery Center in Baltimore. Photo by Doug Kapustin
Lapsed Medicaid coverage barred Mark Pruitt from entering an addiction recovery program last year after he left incarceration, he said.
Mark Pruitt, 46, was released from a Baltimore facility in October with no Medicaid card and a craving for heroin, which he said he had used before he was incarcerated for a parole violation.
He desperately wanted to enter a drug treatment program, but signing up for Medicaid to pay for it was going to take weeks — far longer than he could wait.
“I knew what I wanted. I wanted help,” he said. “I really wanted help. But it’s a struggle when you’re broke — no money, no insurance, feeling defeated. Where do you turn?”
If administrators at a Baltimore recovery facility hadn’t gotten him enrolled in Medicaid, he said, “I think I’d be dead.”
From January 2014, when the Medicaid expansion took effect, through this March, Maryland released almost 16,000 people sentenced to prison or jail, according to state data. Thousands more cycle in and out of jails each year without being convicted.
But the corrections department said it enrolled only 1,337 released inmates in Medicaid from the beginning of 2014 through late March. Another 1,158 prisoners joined Medicaid over that time when they were hospitalized. (Medicaid covers inmates if they spend 24 hours as hospital inpatients; most return to prison.)
Many ex-prisoners are enrolled only when they experience a crisis and end up in an emergency room — the kind of expensive care health officials are trying to reduce. The law requires hospitals to treat emergency cases regardless of insurance coverage. They can retroactively sign those patients for Medicaid.
‘They Don’t Want To Do The Paperwork’
Monique Wright, 35, got out of Jessup Correctional Institution last fall and began suffering acute head and neck pain caused by scoliosis, a spine curvature. Without Medicaid coverage or a doctor, she said she had to seek emergency care at Johns Hopkins Bayview Medical Center.
“It’s the paperwork” that keeps prison officials from making sure people like her have Medicaid upon release, Wright said. “They don’t want to do the paperwork. They don’t have the staff to do the paperwork.”
Advocates wonder why the corrections system is so poor at enrolling what, they often point out, is “literally a captive audience.”
“They’ve had them housed for the past 10, 15 years,” said a frustrated Andre Fisher, a case manager for ex-inmates at Druid Heights Community Development Corp., a nonprofit in West Baltimore. “What’s so hard about it?”
Teressa Jackson learned the prison system hadn’t reactivated her Medicaid eligibility when she got out last year. Jackson called the medical hotline at her Medicaid managed care organization. “They said, ‘There’s nothing we can do because the jail still has a hold on your Medicaid. We can get it lifted but it may take a couple days.’” (Doug Kapustin for KHN)
Jesse Fields is a former inmate who had trouble getting drug-addiction treatment last year. “I couldn’t get on the methadone program because I didn’t have insurance. I was pretty much just out panhandling every day. Holding up a sign, ‘Need Money for Food.’ Anything I could do to get money.” (Doug Kapustin for KHN)
John Whitaker is a former inmate who discovered his Medicaid coverage had expired when he went to the hospital recently. “That’s when the lady said, ‘You know, you’re not covered with insurance.’ I said, ‘Yeah, I’m supposed to be. I got my insurance card…’ She said, ‘No, you’re not in the system right now.’ So she came back up and she put it back through for me again.” (Doug Kapustin for KHN)
Robert Alston is a house manager at A Step Forward, a Baltimore nonprofit supporting recovering drug users. “Sometimes, you know, the system doesn’t send [ex-inmates] home with that monthly supply” of medicine. “So we have to work rapidly if we come across this.” (Doug Kapustin for KHN)
Nichole Franklin is a volunteer for A Step Forward. “You need your health insurance. That’s something you can’t play with.” (Doug Kapustin for KHN)
Travis Howell is a house manager for A Step Forward. When ex-prisoners emerge without insurance, “we have to reapply and take them through the steps. It’s really time consuming, depending on the person. Depending on the situation, it can easily be a month.” (Doug Kapustin for KHN)
Enrolling inmates in Medicaid can take weeks, prison officials said. Sometimes the card doesn’t arrive until after they’re out. Computer problems slowed sign-ups in late 2014.
One mistake made by Maryland and most other states is not considering inmates for Medicaid until their release dates approach, said Colleen Barry, a professor at the Johns Hopkins Bloomberg School of Public Health who has studied the process.
“It’s a bad way to do it because you’re getting a very small number” of enrollees by waiting, she said. A better alternative is to enroll inmates when they are booked, as , she said. Those incarcerated are generally ineligible for Medicaid, but putting them in the system when they enter makes it easier to trigger coverage when they leave, she added.
Ex-Inmates Struggle To Get Medicaid Without Help
If it’s hard for the prison system to enroll inmates, it’s even harder for the individuals to enroll themselves. Those who emerge without Medicaid face a maze of applications, bus trips, phone calls and queues if they want to sign up. Many don’t bother.
For most leaving incarceration, “it’s up to you to go there, make sure you get your health insurance,” said Jamal McCoy, 21, who was living with family in West Baltimore on home detention before he was released. “Most people don’t go. Some people take it easy when they get home.”
Those who try often find that lack of identification is the first challenge. To prevent fraud, Maryland and other states require Medicaid applicants to show verified Social Security numbers.
But jails frequently lose inmate IDs, say prisoners and enrollment officials. Those locked up for years are non-persons for much of the system, with no credit records or driver’s licenses.
That can mean delays of many weeks when released prisoners are especially vulnerable. Gaps in coverage and care of even a few days after fragile patients leave the corrections health system can make the difference between life and death.
“If you’re the diabetic that hasn’t been compliant with your medication, you need your medication now,” said Henrietta Sampson, director of treatment coordination at Powell Recovery Center, a Baltimore addiction recovery agency that works with ex-inmates. “You can’t wait two weeks because you may drop dead.”
BALTIMORE, MD — 3/22/16 — William Carter (50) is from West Baltimore. He is among the men dealing with addiction, and related health issues at Powell Recovery Center in Baltimore. Photo by Doug Kapustin
Prison officials initiated Medicaid enrollment for William Carter when he was released last year. But doctors told him the program wouldn’t cover an expensive hepatitis-C drug until the virus begins damaging his liver.
Compared to the rest of the population, ex-prisoners in Washington state were  in the first two weeks after release, according to research by Dr. Ingrid Binswanger, lead researcher for Kaiser Permanente Colorado’s Institute for Health Research. Drug overdose, cardiovascular disease, homicide and suicide were the leading causes of death.
“It’s very important to manage that transition, to make sure people have continuity of care,” she said. (Kaiser Permanente has no relationship with Kaiser Health News.)
Yet in some cases the prison system has stymied outside groups trying to arrange inmates’ coverage. Stewart’s group repeatedly sought permission — “continuously, for about three years,” she said — to meet vulnerable prisoners inside the facility to get an early start on enrollment and post-release appointments. It never happened.
Baucom blamed the problem on “competing priorities” and staff turnover.
Acceptance into Medicaid by the state isn’t the end of the story. Released inmates then must enroll in a private managed-care organization hired by Maryland to provide coverage. That can take weeks longer.
Even when insured, ex-inmates face the  experienced by other low-income Baltimoreans — or worse.
Many prison inmates are , which can cause liver damage or cancer over time. But the high cost of curing the disease has prompted Maryland’s and other Medicaid programs to to those whose livers are already compromised.
“I guess I got to wait until damage is done to my liver,” said William Carter, 50, adding that prison officials initiated Medicaid enrollment when he got out last year.
Released prisoners often have no idea that some Medicaid managed-care contractors allow them to use only certain doctors and pharmacies.
If you’re the diabetic that hasn’t been compliant with your medication, you need your medication now. You can’t wait two weeks because you may drop dead.
Henrietta Sampson
“So a patient goes to Walgreens or wherever to fill something and it’s like, ‘That’ll be $150,’” because he should have gone somewhere else, said Stewart. “They don’t understand what the problem was.”
Even checking all the right boxes sometimes isn’t enough for ex-inmates, who bear the double stigma of poverty and a criminal history.
One released prisoner got an appointment to renew his mental health prescription with a facility in Carroll County, Maryland — his home — that also accepted his Medicaid card, said Baucom. After the clinic learned he had a prison record it cancelled the visit.
“It’s not enough to have a card,” Baucom said. “You’ve got to have access.”
Neighborhoods are at risk when former inmates with chronic illness return.
“You really need to think about this as a public health issue,” said Scott Nolen, director of drug treatment programs for the Open Society Institute–Baltimore, a nonprofit that works on criminal justice policy. “There is transmission of communicable diseases that happens in prison, in confined spaces. And now those folks are coming back into communities, and we want to make sure they get health care.”
In few places is the burden greater than Sandtown-Winchester. Gray, 25, died of spinal injuries that prosecutors filing manslaughter and assault charges blamed on police who arrested him.
The Justice Policy Institute, a nonprofit, called Sandtown in Baltimore last year, estimating that is in prison.
At the same time, three West Baltimore ZIP codes including Sandtown showed the highest rates of HIV infection in Maryland in 2014, according to hospital data from the Maryland Health Services Cost Review Commission obtained and analyzed by Kaiser Health News and Capital News Service.
The corrections department could use more computers, release planners and other enrollment resources, Baucom said.
“If you do the checkoff list, we’ve checked off everything we can do,” she said, noting efforts to increase enrollment capacity and cooperate with the Maryland motor vehicle agency to get inmates state IDs.
Jesse Jannetta, a specialist at the Urban Institute in prisoner re-entry, believes Maryland’s low sign-up rate “is not unusual” in other states. A found prisons and jails nationwide had enrolled 112,520 people in Medicaid from late 2013 up to January 2015, although the authors believe the actual figure was higher.
Federal and state prisons released 636,000 people in 2014, Millions more to cycle through jails each year.
Few independent experts expect Maryland — let alone most other states — to come anywhere close to full enrollment of emerging inmates anytime soon.
“It’s fair to say we’re just at the tip of the iceberg” in prisoner enrollment, said Johns Hopkins’ Barry, a coauthor of the Health Affairs study. “Maryland is always an innovator. If Maryland is still at the cutting edge of how to do this, many areas of the country don’t have any of these types of programs in place.”
This story is a partnership with The Baltimore Sun and Capital News Service, which is run by the University of Maryland’s Philip Merrill College of Journalism. KHN reporter Shefali Luthra and CNS reporters Catherine Sheffo, Daniel Trielli, Naema Ahmed and Marissa Laliberte contributed.
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=616175&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>616175In West Baltimore, Scarce Pharmacies Leave Health Care Gaps
/public-health/in-west-baltimore-scarce-pharmacies-leave-health-care-gaps/
Mon, 25 Apr 2016 09:00:26 +0000http://khn.org/?p=616179BALTIMORE — The immense new CVS dominates the corner of Pennsylvania and West North avenues. Two smaller pharmacies nearby might both fit inside. One is Keystone Pharmacy, a block away on West North. Care One is five minutes on foot up Pennsylvania.
CVS, its front shelves crammed with brightly-packaged processed foods and household cleaning supplies, is an island of abundance for this West Baltimore neighborhood, .
It’s a contrast that shows what’s changed and what hasn’t in the past year, since Freddie Gray, a 25-year-old black man, died of injuries sustained in police custody, unleashing days of protests. The CVS, just across from the Penn-North metro stop, was on April 27, demolished and rebuilt, opening again just . Looters , though both reopened within days of the protest.
But if 2015’s protests emphasized police brutality and race relations, the absence of more stores like CVS that are easily accessible to people in impoverished, predominantly black neighborhoods underscores Baltimore’s other persistent inequities.
When the CVS was closed, 51-year-old Cornell West said he traveled to a different store, a 30-minute bus ride away. The re-opened pharmacy, where he gets insomnia medicine and cortisone cream, is 10 blocks from his house. (Doug Kapustin for KHN)
Scarcity defines life in Sandtown-Winchester, the 72-block neighborhood where Gray lived for part of his life. Its roughly 9,000 residents are underserved by primary care doctors, by supermarkets that sell healthy food and by full-service retail pharmacies where anyone can pick up a prescription, buy a bottle of aspirin and a few groceries all in the same trip. No major retail pharmacies have outlets inside Sandtown. CVS, the closest to a real grocery store, is near but outside the neighborhood, as are Keystone and Care One, which don’t offer the same variety. Total Health Care, a local community health center, operates two pharmacies on the neighborhood’s border, but they also lack the non-medical variety of a CVS or Rite Aid.
Some of Baltimore’s middle- and upper-class neighborhoods lack these conveniences too, but people there have cars to get where they need to go. Most people in Sandtown must walk or take less-reliable public transportation. That’s a significant barrier for the elderly and those with chronic illnesses. The community has one of the Maryland’s highest rates of hospitalization for .
“There’s not enough quality pharmacy in West Baltimore,” said Jennifer Joseph, director of pharmacy at Total Health Care, which has 10 clinics in Baltimore, six with pharmacies.
That shortfall means disparities in accessing health care persist, despite last year’s outcry.
“Things have returned to normal, but normal still isn’t good enough,” said Anthony Pressley, director of community resources at the Druid Heights Community Development Center. Businesses such as pharmacies and grocery stores aren’t lining up to invest in the area, he added, because they assume it isn’t worth it.
(Story continues below)
Where Pharmacies Are Scarce
In certain Baltimore neighborhoods without retail chain pharmacies — such as CVS, Walgreens and Rite Aid — many residents do not have cars to drive to areas with more stores. Two examples are Sandtown-Winchester and Druid Heights.
Source: Maryland Board of Pharmacy and Baltimore Neighborhood Indicators Alliance. Data analysis by Catherine Sheffo/Capital News Service.
CVS’ 10-month closure posed hardship for some customers. Cornell West, 51, said he took a half-hour bus ride to another CVS for insomnia medication and cortisone cream. Allen Johnson, 61, filled prescriptions at Keystone but couldn’t always get what he needed, he said, such as medications for his knees, blood pressure, cholesterol, heart and diabetes.
“That was a problem for the old people. You know what I’m saying? That was a hell of a problem,” Johnson said.
If we had as many pharmacies as we had liquor stores, it would provide us more opportunity to educate, and promote health and wellness.
Jennifer Joseph
Research suggests that low-income neighborhoods in major cities with higher black and Latino populations are likely to be underserved by pharmacies. A 2014 study in illustrated that pattern in Chicago.
West Baltimore’s shortage of exacerbates the need for pharmacists who can counsel patients about basic health issues. A pharmacist is often the first line of defense for someone with a health condition, said Natalie Eddington, dean of the University of Maryland School of Pharmacy.
“For people who can’t afford health care — they don’t know how to get something,” said Haywood McMorris, the CVS store manager. “They can come here instead of going to the doctor’s and we pretty much take care of it.”
CVS and Keystone compete for that role, but on different scales.
CVS, with 27 stores in Baltimore, is the nation’s largest retail pharmacy chain based on its 9,000 U.S. outlets. It outmatches Keystone, an independent small business, on product variety and supply plus offers better hours. CVS closes at 9 p.m. on weekdays and 6 p.m. on weekends. Keystone closes three hours earlier Monday through Saturday, and it’s closed Sunday. Neither CVS nor Keystone carries fresh produce.
Ellis Basnight, 71, says he relies on the independent Keystone Pharmacy, which is a 15-minute walk from his house. Keystone’s been in the neighborhood for decades, and was one of the stores looted in last spring’s protests. (Doug Kapustin for KHN)
Keystone patrons praise its intimate service and owner Dwayne Weaver’s generosity, sometimes giving them medications on credit when they can’t afford the co-pay.
Argin Henry, 46, shops at both. He goes to CVS for groceries, drinks and goods like toilet paper, but he fills his prescriptions at Keystone, which extends credit when he’s low on cash and delivers prescriptions to his home.
A generous credit policy and delivery service are two ways Keystone competes against its much larger neighbor. CVS is in-network for every Medicaid plan in Maryland. Seven of eight plans cover drugs bought at Keystone, Weaver said. In a week, Keystone might turn away 20 to 25 customers who are out-of-network.
“We kind of survive on servicing patients in a way that chains generally don’t,” he said.
Weaver took over the pharmacy in 1985 and it’s been at its current North Avenue location for about 30 years. CVS has been there since 1997.
Ellis Basnight, who lives a 15-minute walk from Keystone, gets his drugs for diabetes, carpal tunnel and high blood pressure there.
“I’ve been coming here for years!” said Basnight, 71. “That’s why I trust him.”
Weaver considered leaving after last year’s protests. He decided to stay put after neighborhood volunteers helped clean the mess looters left.
The new CVS contains several aisles of over-the-counter medications, a contrast to the much smaller Keystone. As a major national corporation, CVS can offer a wider array of goods than can its independent peers. (Doug Kapustin for KHN)
West Baltimore’s low-income residents do have some alternatives to retail pharmacies, including two clinics of Total Health Care. Patients there can get prescriptions right after seeing the doctor, but retail pharmacies such as CVS can sate their snack cravings too.
Willie Zuber, 50, goes to CVS four blocks from home for groceries and to get medicines for an older woman he said he looks out for. He often grabs a soda or iced tea there while he waits for her prescriptions.
Joseph, Total Health Care’s pharmacy director, said CVS and Keystone likely serve the most people in the area. But they aren’t enough, she added.
“If we had as many pharmacies as we had liquor stores, it would provide us more opportunity to educate, and promote health and wellness, as opposed to alcohol and cigarettes,” she said. “You ride down the streets and what do you see? Abandoned home, abandoned home, abandoned home and liquor store. Bringing that CVS back says a lot for the city.”
Jeremy Snow is a reporter at Capital News Service. CNS reporters Brittany Britto, Ellie Silverman, Catherine Sheffo and Daniel Trielli also contributed. CNS is run by the University of Maryland’s Philip Merrill College of Journalism.
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=616179&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>616179In Freddie Gray’s Neighborhood, The Best Medical Care Is Close But Elusive
/public-health/in-freddie-grays-neighborhood-the-best-medical-care-is-close-but-elusive/
Tue, 16 Feb 2016 10:05:06 +0000The Baltimore health system put Robert Peace back together after a car crash shattered his pelvis. Then it nearly killed him, he says.
A painful bone infection that developed after surgery and a lack of follow-up care landed him in the operating room five more times, kept him homebound for a year and left him with joint damage and a severe limp.
“It’s really hard for me to trust what doctors say,” Peace said, adding that there was little after-hospital care to try to control the infection. “They didn’t do what they were supposed to do.”
Pushed by once-unthinkable shifts in how they are reimbursed, Baltimore’s famous medical institutions say they are trying harder than ever to improve the health of their lower-income neighbors in West Baltimore.
But dozens of interviews with patients, doctors and local leaders show multiple barriers between the community and the glassy hospital towers a few blocks away.
Reporters from Kaiser Health News and the spent much of the fall in and around Sandtown-Winchester, a Baltimore neighborhood where violence flared last year after Freddie Gray was fatally injured in police custody.
Residents say they have little more confidence in the medical system intended to heal them than in the criminal justice system intended to protect them.
It’s really hard for me to trust what doctors say.
Baltimore resident Robert Peace
Even though his accident happened in 2004, Peace says he cannot view doctors and hospitals with anything less than deep suspicion.
“They almost let me die,” he said.
As with so much else, there are two Baltimores when it comes to health. One population is well off and gets the best results from elite institutions on the city’s west and east sides, the University of Maryland Medical Center and the Johns Hopkins Hospital.
The other is a poor minority that gets far less, even as it uses hospital services at higher-than-average rates. One indicator: The typical Sandtown resident lives a decade less than the average American.
“They come in with a great service, but they don’t have relationships with people in the community,” said Louis Wilson, senior pastor of New Song Community Church in Sandtown, a small wedge of . “They want the people in the community to come in and respect them, but they don’t respect the people in the community. It does not work. It just doesn’t.”
The gap is more than the cultural distance between lower-income African-Americans and the wealthier practitioners, often of other ethnicities, who treat them, although that’s a part, Wilson said. It’s about insurance that is still unstable, confusing and perceived as expensive despite the health law’s recent expansion of Medicaid for low-income patients.
It’s about a system that still treats too many residents in the most expensive way possible — in crisis visits to the emergency room — rather than keeping people healthy in the community. It’s about having too few primary-care doctors addressing everyday needs to change that.
It’s about inadequate transportation to get to appointments and jail stays that cut patients off from family doctors. It’s about avoiding medical institutions often seen in the same light as the justice system that held Freddie Gray when he died: as biased, haughty and dangerous.
‘I Lost Two Aunts In That Hospital’
“When you walk into a hospital, it’s like walking into a courtroom,” said William Honablew Jr., who volunteers at LIGHT Health and Wellness, a nonprofit whose community services include helping those with HIV and other chronic illness navigate the system. “You know who’s in charge, and you know who’s not.”
Many in Sandtown have heard of Henrietta Lacks, an African-American woman whose tissue was used without permission by Johns Hopkins Hospital in the 1950s to establish a line of experimental cells. For years Baltimore blacks associated Hopkins, on the city’s east side, with the who supposedly kidnapped black children for medical experiments, residents and community leaders say.
When you walk into a hospital, it’s like walking into a courtroom. You know who’s in charge, and you know who’s not.
William Honablew Jr.
Bon Secours Baltimore Health System, Catholic, nonprofit and the nearest inpatient provider to Sandtown, has reduced potentially deadly, in-hospital hazards such as pneumonia and blood and urinary tract infections in recent years. Adjusted for illness severity, its death rates for Medicare patients with major conditions such as heart failure and stroke are little different from national scores.
But to the frustration of hospital officials who say they deserve better, Bon Secours is still known across West Baltimore as “Bon Se-Killer.”
“I lost two aunts in that hospital, an uncle and two cousins. Five people,” said Arnold Watts, 60, in a grim accounting matched, unprompted, by several other residents interviewed.
The years old, according to the Baltimore City Health Department — .
Detailed data from the Maryland agency that regulates hospital prices, seldom seen by the public, illustrate why.
Residents of the ZIP code including Sandtown accounted for the city’s second- of diabetes-related hospital cases in 2011, the second-highest rate of psychiatric cases, the sixth-highest rate of heart and circulatory cases and the second-highest rate of injury and poisoning cases. Asthma, HIV infection and drug use are common.
born in Sandtown in 2013 were underweight — the highest percentage in any of Baltimore’s 55 neighborhoods. The share of Sandtown mothers getting early prenatal care fell by 25 percentage points in 2013 from the year before.
Dr. Jay Perman is a pediatric gastroenterologist who is president of the University of Maryland, Baltimore, which shares its downtown campus with the University of Maryland Medical Center. Perman, who says the school has a critical role to play in fighting poverty, looks out of his fourteenth-floor, paneled office across a boulevard that marks the beginning of Baltimore’s poor west side.
“Why,” he asks, “in the midst of this extraordinary health care enterprise that is present in Baltimore, with all this expertise, are we sitting here on this side of Martin Luther King (Blvd.) and on the west side of Martin Luther King (Blvd.) you have some of the most disappointing life expectancies that one could imagine?”
Two miles away, residents such as David Johnson start to provide an answer. Johnson, 52, sits in the nave of First Mount Calvary Baptist Church, waiting for food-bank vegetables and talking about being newly out of jail, lacking identification and trying to qualify for Medicaid.
Police arrested Freddie Gray, 25, five blocks from the church last April, allegedly for carrying an illegal switchblade. He died of spinal injuries that prosecutors filing manslaughter charges blamed on police.
Western District police station, where officers removed Gray’s unconscious body from a prisoner van and protesters surged a week later, is a block south.
Pallbearers carry the casket of Freddie Gray to the hearse after his funeral service at New Shiloh Baptist April 27, 2015 in Baltimore. Gray, 25, was arrested for possessing a switchblade knife April 12, 2015 on Baltimore’s west side. According to his attorney, Gray died a week later in the hospital from a severe spinal cord injury he received while in police custody. (Drew Angerer/Getty Images)
Demonstrators face off with Baltimore police as a CVS pharmacy burns at the corner of Pennsylvania and North avenues during violent protests following the funeral of Freddie Gray. (Chip Somodevilla/Getty Images)
A protester walks through tear gas as police enforce a mandatory, citywide curfew on April 28, 2015. (Andrew Burton/Getty Images)
Protesters march on the street from City Hall on May 2, 2015, a day after Baltimore authorities released a report on the death of Freddie Gray. Marilyn Mosby, Baltimore City state’s attorney, ruled the death of Freddie Gray a homicide and that criminal charges would be filed against six Baltimore City Police officers. (Patrick Smith/Getty Images)
A protester holds a sign at the site of the April riots after the mistrial in the trial of Baltimore police Officer William G. Porter on Dec. 16, 2015. The judge declared a mistrial on third day of deliberations in Porter’s trial, which was the first of six trials of police officers involved in the death of Freddie Gray. (Mark Wilson/Getty Images)
A tribute to Freddie Gray marks the site near his arrest in West Baltimore. (Iman Smith/Capital News Service)
Months To Qualify For Medicaid
“I think I have diabetes,” said Johnson. “I know I have high blood pressure. I know that. I get dizzy a lot, especially when I wake up in the morning. I need to see a doctor.”
But he can’t. Baltimore jail authorities lost his identification cards, he said, before releasing him in October from an 11-month stay related to a drug arrest. He spent weeks reapplying for a Motor Vehicle Administration identification card, which social workers said he needed to qualify for Medicaid.
“You need ID to get ID, you know?” he joked. Nobody told him he could use incarceration credentials to qualify.
Medicaid’s expansion to include low-income adults was seen as an unprecedented opportunity to cover former inmates such as Johnson as they rejoin the community. (Inmates are not usually eligible while incarcerated.)
But limited administrative resources for release planning means sign-ups are often limited to the most severely ill, said Lena Hershkovitz, a vice president with HealthCare Access Maryland, a nonprofit working to increase enrollment.
“I know for a fact that he’s not unusual,” she said of Johnson. “I would say the majority of people leaving the prison or detention system are leaving without Medicaid.”
Last year the University of Maryland Medical Center found hepatitis C was causing potentially life-threatening damage to Antonio Davis’ liver, said Janet Gripshover, a nurse practitioner at the Baltimore hospital. Hepatitis C can also cause liver cancer.
Davis’ Medicaid plan, run by UnitedHealthcare, thrice denied doctors’ prescriptions for Harvoni, a new drug that can cure hepatitis C with no side effects but costs up to $90,000 for a full treatment, documents show. Davis, 58, was ineligible because he tested positive for illegal drugs or alcohol, United said in two letters to him.
“I’ve been off drugs and alcohol for six years,” he said, although he acknowledges drugs are probably how he got the virus long ago. “I don’t even drink near beer” — nonalcoholic beer.
Only by switching to a different Medicaid plan, run by Amerigroup, was he approved for Harvoni. Like many states, Maryland contracts with private insurers such as Amerigroup and United to provide Medicaid coverage.
Gripshover and other professionals acknowledge the drug’s high cost but say it saves lives and can save equally large expenses for treating cirrhosis and cancer. “There are no data” to support withholding Harvoni or other treatment from those who use illegal drugs, according to of liver-disease professionals. United declined to comment on his case.
Communication barriers and “poor customer service” are also barriers to care in West Baltimore, according to a , a Boston consultant hired by an association of community health centers.
William Ferebee, 66, has obstructive lung disease and a stent implanted after a 2001 heart attack. He avoids doctors at a University of Maryland Medical Center clinic because “they don’t even really come look at me,” he said. Instead, they give orders to a nurse or resident, “and then he comes in and says, ‘OK, here’s what we’re going to do.’”
A doctor at a nearby, independent clinic “is a sweetheart,” he said. “But it’s so hard to get an appointment.”
Distrust of the system often ensures there’s no communication at all.
Deborah Stevenson, 57, limps so badly with a damaged knee that sometimes people think she’s drunk. She believes she needs a knee replacement, “but I’m scared to get it,” she said. Her orthopedist “wouldn’t answer my questions and deal with me like a patient,” she said.
Even though she doesn’t have diabetes and her leg is otherwise healthy, her son speculated doctors might cut it off.
“I’m handicapped now,” she said. “I don’t want to be crippled.”
Fear of legal consequences also keeps people away from the health system. Some men worry doctors will report their undocumented address to social services, which they believe could reduce aid for female partners who live with them, said Wilson, the New Song pastor.
Medical privacy laws to help law enforcement officials trace suspects and fugitives. Residents subject to outstanding warrants fear they’ll be arrested if they seek care.
“Some people got a case out there — they’re not going to the health clinic,” Wilson said. “They’re going to die without giving up their information.”
Even when patients get access, care is disrupted by physician turnover, poor follow-up or insurance companies’ changing medical networks.
“The system is fragmented,” said Debbie Rock, who has run LIGHT Health and Wellness, on Sandtown’s western edge, since the 1990s. “I think that people need to go back and talk to each other. I think the doctors and the health insurance companies need to sit down and listen to each other.”
One homeless West Baltimore patient left an oral surgeon’s office with a wired jaw and no way to pay for the liquid nutrition he needed to feed himself, said Carol Marsiglia, senior vice president at the Coordinating Center, a nonprofit consulting organization that is working to reduce readmissions and emergency visits in the neighborhood.
A home-oxygen company wouldn’t serve a discharged lung patient because he had a $27 balance, she said. A hospital directed two home-health companies to teach a patient how to deal with a new colostomy bag; neither showed up. The Coordinating Center fixed the breakdowns.
Poverty makes Sandtown’s health worse. Many say poverty causes Sandtown’s poor health.
Four Liquor Stores And Three Sub Shops
Many residents hold jobs in government or manufacturing, run churches or collect pensions from the military or Social Security. Even so, the median Sandtown household
Roofs leak. Mold and mildew grow. Baltimore Gas and Electric cuts off energy to Sandtown households for nonpayment at it does in the rest of the city. Lead paint violations like the kind that are nearly four times higher in Sandtown than in Baltimore as a whole.
Drug and alcohol use are common. Diets are often poor. Many lack cars and the nearest supermarket is more than a mile away from the church.
“If we walk around this block, we’ll pass four liquor stores and three sub shops,” said Derrick DeWitt, pastor of First Mount Calvary, on Fulton Avenue.
Even small co-payments required by many health plans dissuade low-income West Baltimore residents from seeking care, the John Snow report found. Some constantly switch doctors to find the lowest price, leading to “disjointed services” and potential harm if information falls in the cracks, it found.
“I change doctors like I change underwear,” said Eddie Reaves, 64, who tries to find practices that won’t charge him copays as little as $12 or $15. His income is $1,170 a month, he said. In 2014, he added, “I must have seen a good total of about 10 doctors.”
Reaves has diabetes and high-blood pressure. He’s on Medicare because of a disability. He has applied twice to Medicaid since the health law expanded coverage two years ago. That would improve his benefits. But he never received the paperwork, he said.
The best care he ever received, Reaves said, was when he didn’t need any insurance card — when he was homeless.
“I change doctors like I change underwear sometimes” to avoid co-payments as little as $12 or $15, said Eddie Reaves, a diabetic with high blood pressure. Capital News Service photo by Iman Smith.
Health Care for the Homeless, a nonprofit a couple miles east of Sandtown, delivers comprehensive services to the homeless without regard for ability to pay.
“Didn’t have no bills,” Reaves said of the clinic when he used it a few years ago. “Your medicine they helped pay for. They did a lot for you. You could get your teeth done and everything. It was just great, man.”
The rest of the medical system is so unsatisfactory by comparison that low-income Baltimoreans sometimes claim to be homeless when they’re not, just to use the clinic, he said.
What happened after a 2004 car accident that broke Robert Peace’s pelvis is a glaring example of what many say is the kind of medicine that has been practiced too long in West Baltimore and what many say they are working to change.
Emergency surgery at UMMC fixed the fracture. But Peace developed a persistent bone infection. He received little or no follow-up care, he said, getting treatment only when the infection surged out of control and required repeated, expensive surgeries.
“The pain would be so intense — it’s like, wracking my body. I would literally sit there and shake,” he said. “That’s when I would know I had to go to the hospital, because I knew the infection was back.”
He said he required five more surgeries over a year and a half — the kind of return trips to the hospital, or “readmissions,” that the health industry and the Affordable Care Act of 2010 are trying to reduce by promoting coordination between hospitals and community doctors.
Robert Peace, outside the home of his brother in Northeast Baltimore on Jan. 15, 2016. (Doug Kapustin for KHN)
“I’m blaming it on the follow-up,” said Peace, 58. “They knew the infection wasn’t going away, but the only time they would really tend to it was when I was in the hospital.”
Today Peace walks with a cane and a pronounced limp.
It’s a story that’s still too common in West Baltimore, said Antoine Bennett, a lifelong Sandtown resident and an elder at New Song Community Church.
“We’ve got a joke here, but it’s a serious joke,” he said. “If they ain’t medicating, they’re amputating or operating. But what’s missing is the care. Primary care.”
When asked about Peace’s case, UMMC spokesman Michael Schwartzberg said, “Much has changed in the Maryland hospital environment” since his surgeries. Improvements include new emphasis on preventing readmissions and “significant investment” in care coordinators and other post-discharge management, he said.
Keeping People Healthy And Out Of The Hospital
By many accounts, hospitals, doctors, health plans and governments in Annapolis, Maryland’s capital, and Washington are making unprecedented efforts to bridge the medical divide with Sandtown and the rest of low-income Baltimore.
The grand idea is to save money and simultaneously improve lives by keeping people healthier in the community instead of letting them become ill enough to land in the hospital.
In October Bon Secours that it intends to turn into a primary care and wellness center. UMMC and Bon Secours are working with “transition coaches” from the Coordinating Center to make sure people leaving the hospitals take medicine and schedule follow-up appointments. UMMC’s transition clinic serves hundreds of recently discharged patients.
Maryland is developing one of the most advanced electronic networks for letting medical providers collaborate by sharing patient records. Health Care for the Homeless in Bon Secours.
Dr. Samuel Ross, Bon Secours’ CEO, talks about working more closely with the churches and continuing to improve the hospital’s outcomes and reputation.
BALTIMORE, MD — 2/12/16 — Dr. Samuel Ross, CEO of Bon Secures Hospital in Baltimore, Maryland. Photo by Doug Kapustin
“No, it’s not solved,” he said. “We need to keep doing what we’re doing, and understand that some of this is a person at a time. There is no wholesale campaign or branding message that’s going to cause people to say, ‘You’re wonderful.’”
In 2012 Maryland’s legislature created “health enterprise zones” to increase the supply of primary caregivers in West Baltimore and other underserved areas. UMMC puts emergency room patients in touch with a primary care doctor if they don’t have one.
In September hospitals proposed taxing insurance companies, employers and other payers so they could hire up to 1,000 caregivers directly from West Baltimore and other low-income communities with poor health results.
The Baltimore health department is pressing hospitals to collaborate on high-risk patients and is building ties with lower-income neighborhoods by hiring residents, said Dr. Leana Wen, the city’s health commissioner.
Baltimore’s B’more for Healthy Babies program has the city’s African-American infant mortality rate by nearly a third , to 12.8 per thousand births. But that’s still a fifth higher than the African-American rate for all of Maryland.
University of Maryland Medical Center has for high schoolers interested in health careers. The University of Maryland, Baltimore, got a to increase the number of African-Americans in health care jobs.
More and more professionals echo UMB’s Perman, who said a medical professional’s duty to patients does not end at the hospital or clinic door.
“As a profession, as an industry, we have not sufficiently appreciated, let alone done something about, the impact of social determinants” such as poverty, poor housing, lack of food choices and low education, he said. “Guys like me and gals like me can easily say, ‘I made the correct diagnosis. I wrote a proper prescription. I’m done.’ What I say to my students is, if you think you’re done — if ‘done’ means the patient is going to get better — you’re fooling yourself.”
Maryland’s ambitious overhaul of hospital reimbursement, authorized by the health law, is supposed to back that philosophy with powerful incentives. Starting in 2014, hospitals have been assigned annual budgets for all government and private payers, instead of being paid per admission or treatment.
The idea is to boost their motivation to contain costs by delivering preventive, community care — to pay them for keeping people out of the hospital. Hospitals are also getting penalized for excessive readmissions and preventable harm such as infections and accidental punctures.
“It’s a daunting task… when we talk about joblessness and poor nutrition and violence in the neighborhoods,” said Dr. Walter Ettinger, chief medical officer of the University of Maryland Medical System. “But we all feel driven by our mission to serve our communities in a better way, and now the finances are aligned to do that.”
Poor people, however, know that between ambitions and accomplishments is a chasm of disappointment.
In the face of wider primary-care shortages and the difficulty for doctors to make a living in low-income neighborhoods, the zone fell far short of its original goal of to West Baltimore.
“Some of the goals and objectives across almost all of the zones were a bit ambitious,” said Maura Dwyer, a senior policy advisor for the Maryland Department of Health and Mental Hygiene.
In 2014 People’s Community Health Center in Baltimore and later entered bankruptcy proceedings, demonstrating the difficulty.
Total Health Care operates several federally qualified health centers in Baltimore. (Iman Smith/Capital News Service)
Officials at Total Health Care, a federally supported nonprofit with several primary-care clinics near Sandtown, say they are proud of their service to West Baltimore.
“We want to bring the standard health in this neighborhood up to national standards,” Dr. Marcia Cort, Total’s chief medical officer, told students from the Merrill College. “We don’t want it to be the neighborhood and area [where] life expectancy is low and people are dying from preventable things.”
Still, she said, “Baltimore City is in a health crisis.”
Readmission rates for Bon Secours were still in 2014, although the Coordinating Center’s transition coaches helped reduce them by 14 percent from the year before.
Readmissions for UMMC’s midtown campus were second highest statewide after declining 5 percent, also with work by transition coaches. At UMMC’s downtown campus, readmissions were fifth highest in the state and declined 2 percent.
But state financing to pay for the transition coaches expires at the end of March. The Coordinating Center is optimistic it will be renewed but nothing is set, Marsiglia said.
In 2014 only that they understood their care after they left the hospital. For UMMC patients the figure was 51 percent.
Many resent that it took this long for the industry to try the very solutions — improving primary care, giving communities resources to help themselves — that residents of neighborhoods like Sandtown have been advocating for years.
“Unfortunately the hospitals didn’t hear us,” said Diane Bell-McKoy, CEO of Associated Black Charities, a Maryland nonprofit. “As a person of color giving that information — most people think we don’t know what we’re talking about.”
Distrust of the system, still more widespread than medical officials imagine, is passing to a new generation, residents say.
“It’s a culture that has come about over time, because younger people have seen or feel like their parents and their grandparents didn’t get the best medical treatment when they went to the hospital,” said First Mount Calvary’s DeWitt. “So they have this why-go attitude.”
Derrick DeWitt is the pastor of First Mount Calvary on Fulton Avenue in Sandtown.
On Dec. 9, Maryland regulators made three months earlier to create hospital jobs in poorer neighborhoods.
Other initiatives do little to address the low incomes and unemployment linked to Sandtown’s poor health. Nor do they simplify the shifting maze of private and government insurance plans and hospital and doctor networks that patients must navigate to get care.
One example: Nearly 2,000 low-income Medicaid members, including many in Sandtown and nearby, had to change coverage in August or get new doctors because United dropped University of Maryland Faculty Physicians from its Medicaid network in a contract dispute, said Shannon McMahon, deputy secretary of the Maryland Department of Health and Mental Hygiene.
United “had thorough continuity of care measures in place before the contract ended to ensure ongoing care was not disrupted,” said company spokesman Ben Goldstein.
For many residents, enrolling in a plan is too complicated and time-consuming, requiring time off from work to get coverage they don’t understand and can’t afford, said LIGHT Health’s Rock. In some ways the health law and its new coverage rules have made things more complex, she said.
“As the landscape is changing, people really just don’t know what to do,” she said. “They sit you down with somebody that’s supposed to help you fill [an insurance application] out, which is like a Charlie Brown episode. Once you start on the second page it’s like ‘Wah, wah, wah.’ You don’t hear nothing else. You walk out and it’s like, ‘What happened?’”
David Johnson, who was concerned about his blood pressure, dizziness and possible diabetes, joined Medicaid in December. It took two months, three trips to the motor vehicle bureau to get a new ID and two trips to social services to enroll.
An still hadn’t signed up for Medicaid as of October. As of early February, Eddie Reaves, the diabetic who gave up applying after his second attempt, was still among them.
This story is part of a reporting partnership between and University of Maryland College Park’s , which operates Capital News Service. KHN and students from the school are examining how Baltimore’s nationally respected health system serves the community where violence flared in April after Freddie Gray was fatally injured in police custody. The project is continuing. To see all the students’ work go to the .
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
<img id="republication-tracker-tool-source" src="/?republication-pixel=true&post=600143&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>600143Video: Baltimore Hospitals Work To Repair Frayed Trust In Black Communities
/public-health/video-health-problems-fester-in-freddie-grays-neighborhood/
Tue, 16 Feb 2016 10:00:53 +0000http://khn.org/?p=599801In a city renowned for medical schools and research, there’s a striking contrast in the dismal health and life expectancy in some Baltimore neighborhoods. There’s a deep distrust of the medical system among many African-American residents, dating back to the 1800s. Kaiser Health News’ Sarah Varney reports on efforts to repair the relationship, as part of a collaboration with .
Â鶹ŮÓÅ Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Â鶹ŮÓÅ—an independent source of health policy research, polling, and journalism. Learn more about .
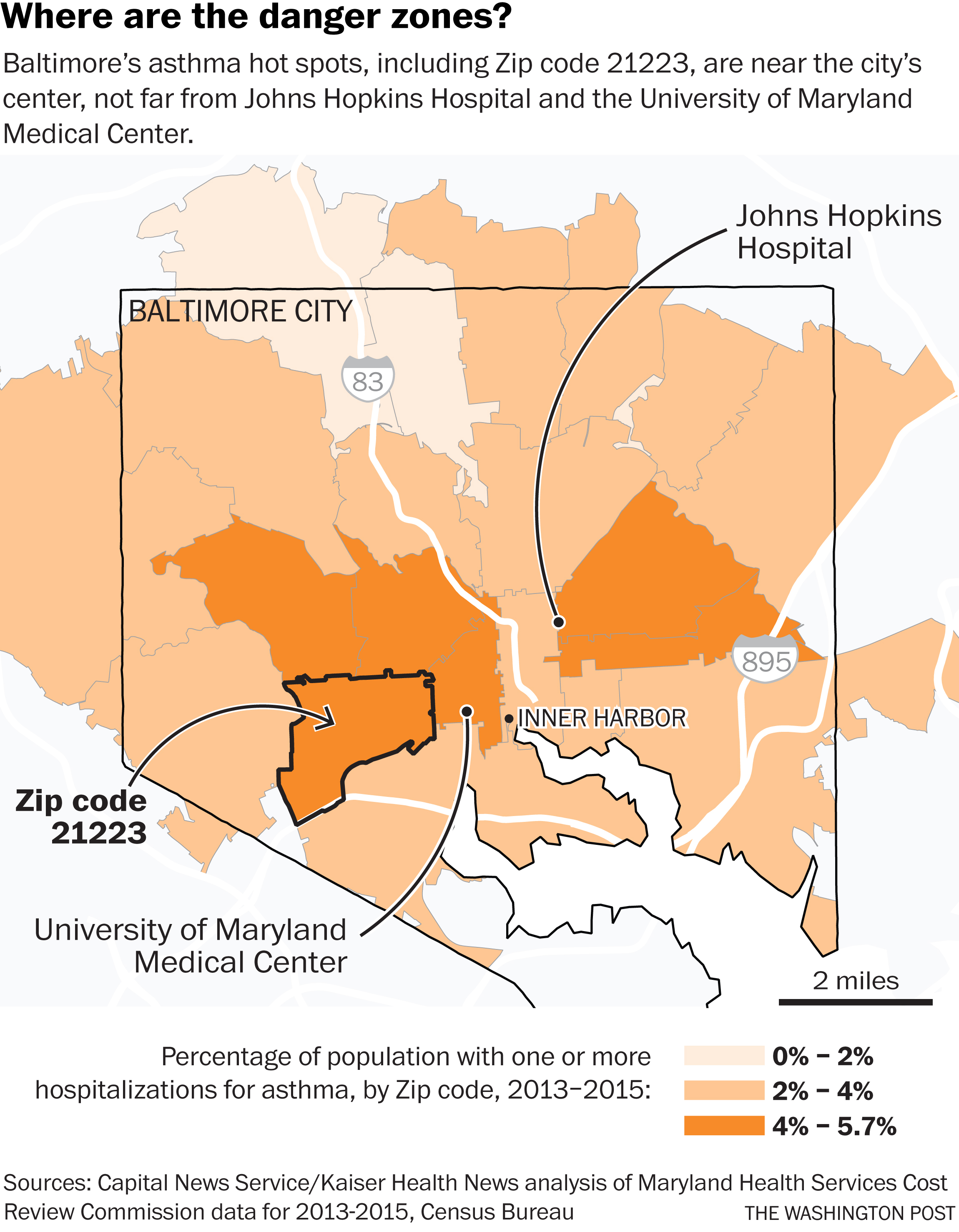




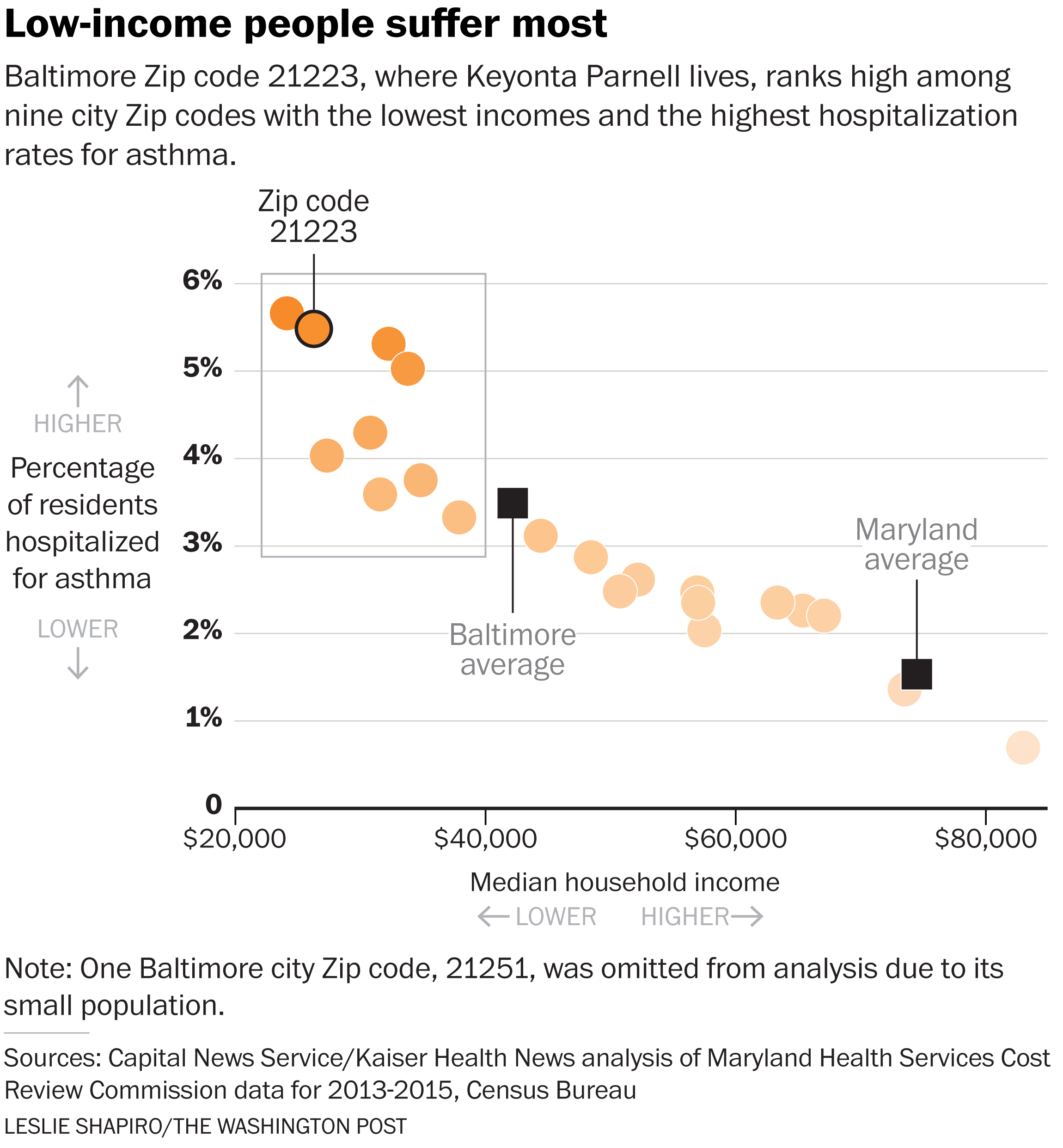
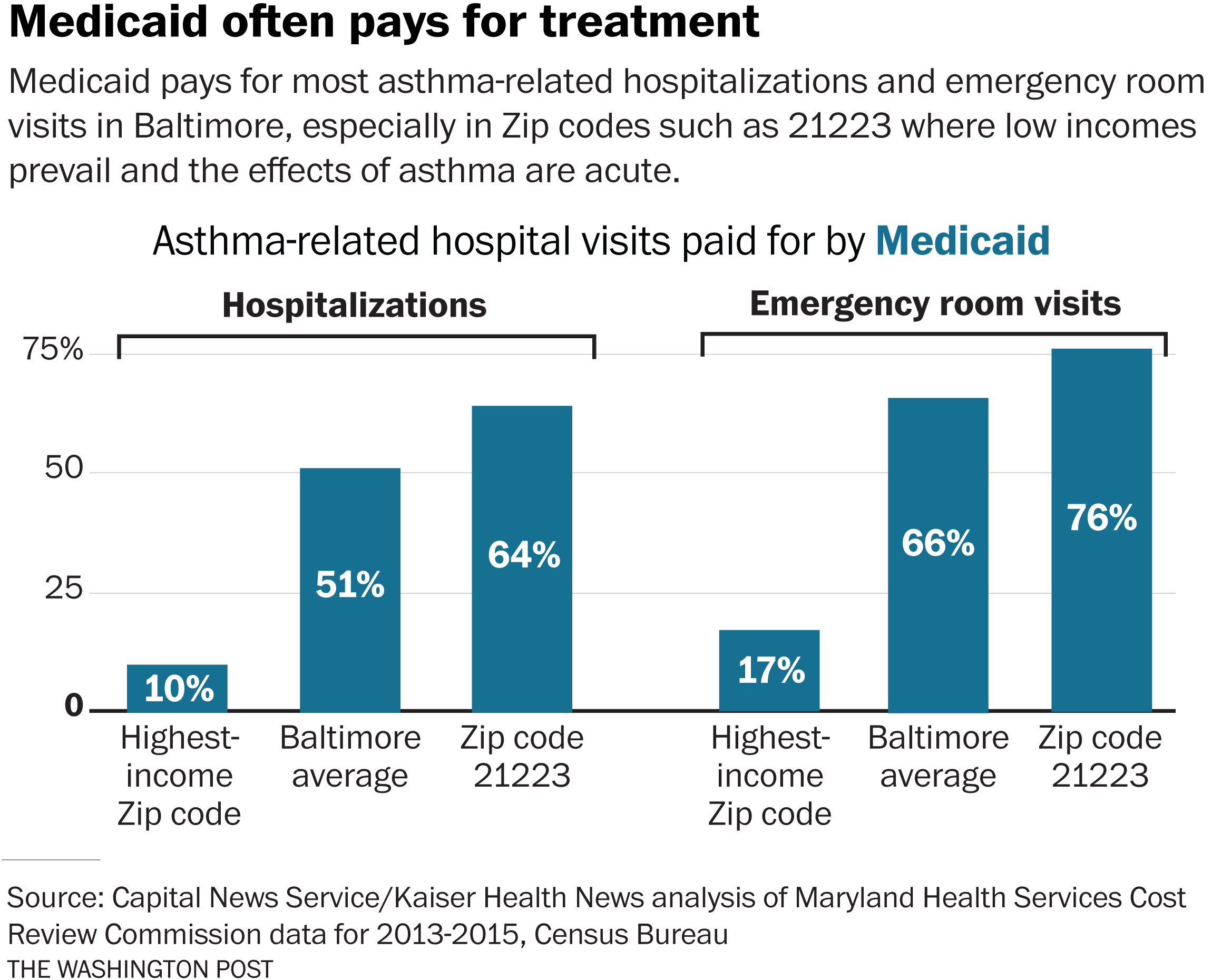
{kind=link}